Download
1 / 17
180 likes | 374 Views
Anatomia microchirurgica della regione temporo-silviana. Studio anatomico preoperatorio: Tips and Tricks Neurochirurgia - San Giovanni-Addolorata - Roma Massimiliano Neroni. Insular anatomy After opening the temporal and fronto-parietal opercula.

E N D
Anatomia microchirurgica della regione temporo-silviana. Studio anatomico preoperatorio:Tips and Tricks Neurochirurgia - San Giovanni-Addolorata - RomaMassimiliano Neroni
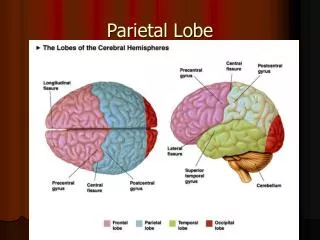
Insular anatomy After opening the temporal and fronto-parietal opercula
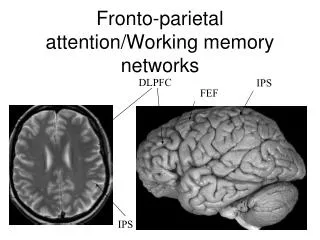
Knownledge of the phylogenesis of the structures Mesiobasal temporal Temporal pole Amygdala Limbic Hippocampus Parahippocampus 2 layered structures (allocortex) Cingulate Gyrus Fornix Paralimbic Mammillary body Caudal Fronto-Orbital Gyrus (included Pars Orbitalis) INSULA 3-5 layered structures (mesocortex)
Preferential brain locations of LGGDuffau H. and Capelle L. Cancer, 2004 Jun 15;100:2622-666% insular tumor are LGG LGG are more likely located in “secondary” functional areas immediately near to the so called “eloquent areas”. Insula is a part of the mesocortex with 3-5 neuronal layers (Paralymbic region: M.G. Yasargil et al: Microsurgery of Insular Gliomas) LGGs show an affinity to phylogenetically more primitive zones. Fillimorf 1947 and then Yakovlev in 1959
T2 sharp imaging on benign tumorM.G.Yasargil,Ali F. Krisht, Ugur Ture, Ossama Al-Mefty and D.C.H.Yasargil Microsurgery of insular glioma Part III – Contemporary Neurosurgery 24;13:1-6Y.A. Moshel, J.D.S. Marcus, E.C. Parker and P.J. Kelly Resection of insular gliomas: the importance of lenticulostriate artery position. Clinical article. JNS November 2008;109:5
Lesion displacing LSAs medially often represent a sharp-well demarcated T2 MR images and LGGs histology. On 429 Limbic-Paralimbic tumors31/191 of the Insular Gliomas demostrated anaplastic grade (MG Yasargil Microsurgery of the insular gliomas on Cont. Neurosurg. VOL. 24,14:JUL 15.2002)Tumor with moderate shift of the LSAs and T2 MR images showing a diffuse boundaries pattern are most likely HGG and aggressive surgery is often associated to permanent deficit.
Y.A. Moshel, J.D.S. Marcus, E.C. Parker and P.J. Kelly Resection of insular gliomas: the importance of lenticulostriate artery position. Clinical article. JNS November 2008;109:5 - 50% patients underwent previous surgery in other institutions - 70% patients presenting with seizures - 20% with mild hemiparesis - 45% pure insular tumors (55% with opercular extension) - 20% High enhancing lesion with high grade tumor: had postop permanent deficit ((30% TGR) - 80% Low enhancing lesion were LGGs (70% TGR was achieved) - - Opening the sylvian fessure at the sylvian center - Dethetering of M4-M5 vessels - Without metal retractors - Depending on the target: multiple vertical incision dividing the M2-M3 branches - If present opercular extension first approached - MEP and SEEP are strictly necessary only in the dominant hemisphere Tumor approach
Methodics & Tools- MR - Functional MR- Intra-op Ultrasound- PET (tumor grade)- Intra-op vascular microdoppler- DS Angiography demonstrating the LSA displacement- Intra-op evoked potential recording (internal capsule)- Awake surgery preferred in the dominant hemisphere
M.G. Yasargil lesionectomy for insular tumors 1) Removal of the central zone performing a longitudinal sulcus incision2) Debulking of infero-anterior zone3) Debulking of the inferior region4,5,6) Once obtained room enough: antero-superior, superior and posterior7) Removal of the region in the limen insula
Fuctional MR demonstrating the tumor boundaries and the Uditive area without pallido-capsular involvement
Functional MR demonstating temporal opercular region tumor involvement and uditive area to avoid during the tumor approach (no distraction of the opercula)
Tractography of capsula interna axial view andtemporal opercular uditive area in right hemisphere
MR Tractography recognizing tumor boundaries without involvement of the capsula interna 3D MR with surface imaging demonstraing no encasement of the putamen GP, NC and CI.
Tumor LSAs medial displacementOpen biopsy: anaplastic glioma Anaplastic Astrocytoma: atypia, ipercellularity and mitosis (WHO III)