Download

1 / 19
200 likes | 396 Views
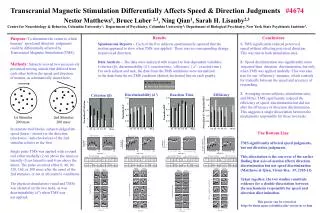
Dec 7, 2012. Continuous Repetitive Transcranial Magnetic Stimulation for intractable Neuropathic Pain. Youichi Saitoh , M.D., Ph.D. Department of Neuromodulation and Neurosurgery Office for Univeristy -Industry Collaboration, Osaka University.

E N D
Dec 7, 2012 Continuous Repetitive Transcranial Magnetic Stimulation for intractable Neuropathic Pain YouichiSaitoh, M.D., Ph.D. Department of Neuromodulation and Neurosurgery Office for Univeristy-Industry Collaboration, Osaka University
Electrical motor cortex stimulation; EMCS EMCS expand to the world from Japan Rasche et al., Pain, 2006 Saitoh et al. J Neurosurg 2000 Department of Neurosurgery, Osaka University Graduate School of Medicine
Efficacy of EMCS on intractable neuropathic pain Approximately half of the patients satisfy No large double-blinded clinical trials Saitoh and Yoshimine, ActaNeurochirSuppl, 2007 Saitoh Y et al, ActaNeurochir, 2007
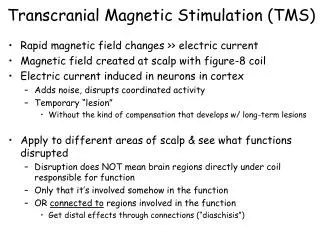
Repetitive transcranial magnetic stimulation(rTMS) Eddy current curent Figure-8-coil is most popular
Cochrane reviewO’Connell NE et al, 2010Non-invasive brain stimulation techniques for chronic pain • Single doses of high-frequency rTMS of motor cortex may have short-term effects on chronic pain. • Efficacies of cranial electrotherapy stimulation and transcranial direct current stimulation are uncertain. VS
Multi-centered, Randomized, double-blind, sham-controlled, crossover study2009 〜2011 This study was funded by the Japanese Ministry of Health, Labourand Welfare with a Health and Labour Sciences Research Grant.
Randomized, double-blind, sham-controlled, crossover study • Real (5Hz)and sham stimulations are randomized. • Double-blind Randomized Crossover Study • Specialist of biological statistics randomized the patients to two groups. • Validation of efficacy and safety of daily rTMS for 2 weeks. • Previous studies were mostly single session • Primary endpoint is VAS, secondary is SF-MPQ • Realistic shamis applied. • Synchronized cutaneous electrical stimulation is delivered. • Hamada M et al, MovDisord, 23:1524-31, 2008 • 70 patients
Randomized, double-blind, sham-controlled, crossover study • Seven centers • Rehabilitation, Hokaido Univ. • Neurology, Fukushima • Neurosurgery, Nihon Univ. • Neurosurgery, Hamamatsu Univ. • Neurosurgery, Osaka Univ. • Neurology, Kinki Univ. • Neurology, Univ. of Occulational
Trial profile Sham first Real first
Patient global impression of change (PGIC) Intervention
Beck depression inventory (BDI) Intervention
Discussion • This prospective study shows daily high-frequency rTMS is transiently effective for pain relief in intractable neuropathic pain patients (70 cases). • There has been no serious adverse effects. • The real rTMS, compared with the sham, showed significant short-term improvements in VAS and SF-MPQ scores without a carry-over effect. The result of PGIC suggested cumulative effect. • More than once a day or continuous rTMS treatment may improve the effect. • In this study, 81% of enrolled patients were post-stroke pain and 60.7 y.o. (mean) which is older than previous studies. Therefore, the effect was mild but significant.
Cerebral mechanism of pain relief(EMCS, rTMS) rTMS M1 ACC S2 Modulate pain recognition PFC Ins Th Pain relief PAG Modulate a pain threshold Elicit plastic changes