Download
1 / 36
430 likes | 744 Views
Tibialis posterior tendinopathy. Dr F Pato February 2012. Patient history. 31year old male patient Weight 97kg, height 1.79m, BMI 30.27 Review of a painful right foot and ankle Half Iron man April 18months 40km a day Training shoe: Nike Pegasus. Complains of:

E N D
Tibialis posterior tendinopathy Dr F Pato February 2012
Patient history • 31year old male patient • Weight 97kg, height 1.79m, BMI 30.27 • Review of a painful right foot and ankle • Half Iron man • April • 18months • 40km a day • Training shoe: Nike Pegasus
Complains of: • the knee pain has improved • foot pain still persisting
Examination • Tenderness • medial aspect of right ankle • posterior to the malleolus • Tinel test negative • Knee joint • Minimal tenderness over the medial joint space and below • Biomechanichal assessment • Static and dynamic evaluation • Core stability assessment • Gait assessment
Assessment • Tibialis posterior tendinopathy • Tarsal tunnel syndrome • Plantar fasciitis • Tibialis posterior tendinopathy with minor forefoot eversion/ pronation and poor hip stability.
Management • Inner foot soles • Physiotherapy referral • Biokinetics referral
Aim of management • Stabilisation • Proximally: core stability • Distally: inner foot sole • Inner foot sole • Foot arch support • Muscle support • Stabilizing of pelvis • decreases the pressure on the medial leg • Deloading the medial aspect of the foot • Core stability training and muscle training and conditioning for running • Reduce excessive muscular activity present in high degrees of overpronation
Discussiontbp t mx • Primary dynamic stabiliser of medial longitudinal foot arch • High forces act on tendon • Influenced by adverse biomechanics in overpronated foot • Overuse injury • as a result of excessive walking, running, jumping • overuse injury than acute traumatic injury • High degrees of subtalar joint overpronation lead to the development of this problem • Excessive activity of tibialis posterior muscle in ankle overpronation (subtalar joint)
Excessive subtalar pronation • increased eccentric tendon loading during supination for the toe-off phase • Acute • direct or indirect trauma • avulsion fracture • Inflammatory conditions: • tenosynovitis secondary to rheumatoid arthritis • seronegativearthropathies • Chronic tendinopathy • rupture of the tendon itself • collagen disarray • interstitial tears
Overuse of the tibialis posterior muscle and long flexor tendons results in trauma to the periosteum and bending of the tibia. • Chronic overloading can also result in fibular stress fractures.
Historically • Two main theories • Mechanical • Vascular • Neural theory emerging • Mechanical theory • repeated loading causes fatigue and tendon failure • degenerative in nature • increases with age • Vascular theory • Metabolically active tissue • Requires vascular supply • Lack thereof causes degeneration
Neural theory • tendons are innervated tissue • Close association of nerve cell endings and mast cells within tendon • Neurally mediated mast cell degranulation • Chronic overuse • Excessive neural stimulation and mast cell degranulation • Substance P pro-inflammatory • Glutamamate in Achilles tendinopathy • Combination of above factors
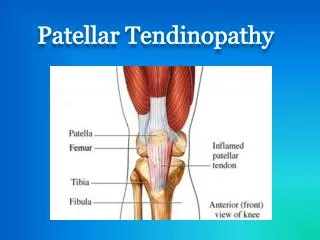
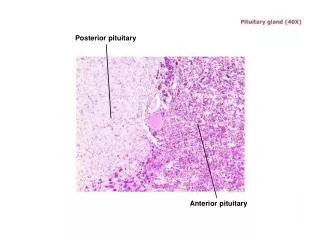
Anatomy • The tibialis posterior muscle tendon • inverts the subtalar joint. • stabilizes the hindfoot against valgus forces • provides stability to the plantar foot arch • Tarsal tunnel • Anatomical structure on inside of heel bone • Tendons from calf to toes • FHL,FD,TP • Posterior tibial nerve • Tibialis posterior tendon is palpated from the posteromedial to the medial malleolus, insertion point is at the navicular tubercle.
Macroscopic appearance • Disorganised tissue • Mucoid degeneration • Collagen degeneration • Fibrosis • Neovascularisation • Increased fibroblasts • Increased Prostaglandin E2 production • Leucotriene B4 • Degenerative change
Biomechanics of running • Correct biomechanics result in • provision of sufficient movement • reduction of risk of injury. • Non traumatic sport injuries can potentially be caused by • abnormal biomechanics. • Static (anatomical) • functional (secondary) • Static abnormalities cannot be altered • Secondary effects altered by means of orthoses • Poor technique and previous injury can result in functional abnormalities • Muscle imbalance • Joint laxity
The range of motion of the ankle joint • ±45o plantarflexion • Neutral when the foot is perpendicular to the leg. • The minimum range of motion required for movement • is 10-20o for normal walking
Excessive pronation results in • excessive internal rotation of the entire lower limb during weight bearing, • thus increasing demands on numerous structures. • The subtalarjoint • region where pronation occurs • This leads to • ground reaction forces being increased on the medial aspect of the foot. • the foot therefore becomes unstable.
The medial longitudinal arch also receives excess loading causing increased strain on the plantar fascia and musculature. • The supporting muscle ends up contracting harder and longer to decelerate rotation and pronation of the foot. • Muscles involved is the • gastrocnemius-soleus complex • tibialisposterior. • May result in • Achilles tendinopathy • tibialis posterior tendinopathy.
Excessive pronation results in increased rotation of the tibia, resulting in : • Patella being laterally sublaxed • Quadriceps muscle imbalance • patellofemoral joint dysfunction • Predisposition to patella tendinopathy • Tightening of the iliotibial band • Tibial stress fractures
Clinical picture • Medial ankle pain • behind the medial malleolus • Extending to tendon insertion point • Swelling is unusual • There is tenderness along the tendon with occasional presence of crepitus • With resisted inversion • relative weakness compared to the contralateral side • eliciting of pain • There is lack of inversion of the hind foot • difficult to perform a heel raise.
Investigations • Magnetic resonance imaging (MRI) • Sensitive and specific for detection of rupture is high • 80% and 90% • Extent of tendinosis is revealed • Most useful method of imaging tendons around the ankle • Ultrasonography • Less sensitive than MRI • Inflammation • Serology and inflammatory markers • blood
Management • Conservative versus Surgical • Conservative • Pain control where necessary • Ice if necessary • Eccentric and concentric tendon loading exercises • Soft tissue therapy • Manual • Stretching Reteaching of balance and proprioception
Rigid orthoses • excessive pronation controls • Symptomatic relief • Anti-inflammatories • If caused by inflammatory arthropathies • Immobilization • If severe • Cast used for short term relief of symptoms • Surgical • If failed conservative • ?reconstruction
Concentric training • Active shortening of muscle tendon unit • Eccentric training • Active lenghteningof muscle tendon unit • Alfredson’s protocol • Painful heel drop protocol • Achilles tendinopathy • 12weeks
Soft tissue therapy • Restore pain free range of movement • Joints • Muscle • Tendon • Nerves • Explain to patient beforehand
Massage • Assess abnormal tension regions • Trigger points • Systemic palpation • Position of treatment • Target tissue • Under tension or laxity • Balance and proprioception retraining
Digital ischaemic pressure • Evoke temporary ischaemic reaction • Stimulate tension monitoring receptors • Reduce muscle tone • Release of pain mediating substances • Analgesic response • Deactivate symptomatic trigger points
Sustained myofascial tension • Application of tensile forces in direction of greatest fascial restriction or in direction of elongation necessary for normal function • Aim is to rupture abnormal cross linkages between collagen fibers • Cross linkages form aro inflammatory response to acute or overuse injury • Depth of treatment • Granter-King scale • Pain grade I – IV • Resistance grade A-C
Orthoses • Correction of mechanics and alignment • Compensation of structural abnormalities • Controls excessive subtalar and midtarsal movements • Placed in the shoe • Must not be used alone • Types of orthoses • Preformed • casted
Preformed • Flexible • Provides conservative control of foot motion • establishes tolerance to posture changes • Determine: control of motion, assist in injury management • Gives indication if rigid ones will be necessary or helpful to treat lower limb problems • EVA • cork • rubber • plasterzote • polyurethane
Catsed • Polyurethane • Carbon fibre deposits • Alter foot mechanics significantly • Importance is the awareness of the individual’s tolerance to change inner mechanics.
Future • Stem cells ?
Prevention • Corectionof biomechanics • Two methods of correcting lower limb biomechanics • Proximal distal correction • Proximal : correction of poor pelvic mechanisms • Distal : foot orthoses and footwear • Muscle weakness or incoordination • Strengthening and retraining • Joint stiffness • Active and passive joint mobilization • Appropriate shoes
Conclucsion • A chain is as strong as its weakest link • Injuries in one part of the kinetic chain result in dysfunction of the whole chain • Injuries and adaptations in some area of the kinetic chain can result in problems distant from the affected area. • compensate for the inadequacy in order to generate adequate force to perform a specific task. • Identification and correction of deficits important to prevent further injury • Proper function of chain • Performance • Multi team approach rehab programme • Well planned • Well excecuted • Individualised
Refrences • Brukner and Khan. Clinical Sports Medicine Revised Third Edition.2010;40-61, 129-151,600,634-637 • Tim Noakes.Lore of running. 4th Edition, 2001 • Current concepts in management of tendon disorders.JD Rees.Rheumatology.May 2006:45(5):508-521 • Non surgical management of posterior tibial tendon dysfunction with orthoses and resistive exercise: A randomized Controlled Trial. Journal of the American Physical Therapy Association. Kulig et al.January;89(1):26-37 • Does Eccentric Exercise Reduce Pain and Improve Strength in Physically Active Adults With Symptomatic Lower Extremity Tendinosis? A Systematic Review.NJ Wasielewski et al. Journal of Athletic Training. 2007 Jul-Sep;42(3):409-421