Download
1 / 83
840 likes | 1.04k Views
CKD & OBSTRUCTIVE UROPATHY Jan23-24 2012@PNAN, Ile-Ife. Felicia Eke, MD University of Port Harcourt Nigeria. Outline. 1. Definition CKD & Obstr Uropathy Mechanism Obstr.Urop CKD Case presentations Quiz Management. Definition-Obstructive Uropathy.

E N D
CKD & OBSTRUCTIVE UROPATHYJan23-24 2012@PNAN, Ile-Ife Felicia Eke, MD • University of Port Harcourt • Nigeria
Outline • 1. Definition CKD & Obstr Uropathy • Mechanism Obstr.UropCKD • Case presentations • Quiz • Management
Definition-Obstructive Uropathy • Obstruction anywhere down the Urinary tract
** ** ** ** Stages of CKD—KDOQI, 2002 *Kidney damage for >3 months, as defined by pathologic abnormalities or markers of kidney damage, including abnormalities in blood or urine or diagnostic imaging studies.
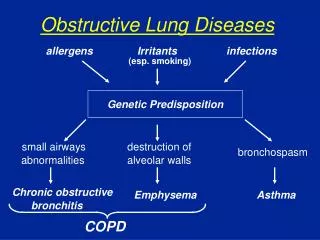
TYPES OF OBSTRUCTIVE UROPATHY • A: MECHANICAL OBSTRUCTION • B: NON-MECHANICAL- FUNCTIONAL
Mech:Developmental Anomalies • Posterior Urethral Valves • Pelvi-ureteric Junction Obstruction • Ureteric Stricture • Ureterocoele • Tumours-Rhabdomyosarcoma • Ureteric & Bladder stones- Cystinuria • Meatal stenosis • Distal urethral stenosis • Cystic malformations, • Duplex • Dysplastic Kidneys
Mech: Acquired Anomalies • Tumours • Bladder & ureteric stones- Melamine stones from Infant formula
Functional: Damaged kidneysCKD • Vesico-Ureteric Reflux • Spina Bifida • Myelomeningocoele • Neurogenic bladder eg from Prune belly etc
PUV: Case 1-PO • One of v. few success stories of PUV • Noted at birth to have poor urine stream • Big abdomen-bladder • Both kidneys enlarged
Posterior Urethral valves(PUV) • Entire urinary tract develops in environment of high intraluminal pressure from • Obstruction Cell apoptosis, inflammation • Permanent defects - parenchymal dysplasia of kidneys, ureters, bladder despite adequate decompression of the urinary tract pre or post natally
PATHOPHYSIOLOGY (cont) • In some, renal tubules mainly affected poor urine concentrating ability, diuresis ureteral & bladder dysfunction • Affected kidneys may function well initially, but have a reduced renal reserve • Renal deterioration also frm chronic pyelonephritis from Vesicoureteric (V-U) reflux, urinary stasis
PUV Clinical Presentation • Extremely variable • Prenatal US :Oligohydramnios hyroureters, hydronephrosis • Respiratory distress-pulmonary hypoplasia • Potter’s facies, ascites, and abdominal swelling • Birth: Poor, dribbling urine stream • So check urine stream of all males b/4 discharge from hospital
PUV Clinical Presentation • Toddlers - voiding dysfunction or UTI • School-aged boys usually come to the clinician's attention because of urinary incontinence • All enuretics should be screened at least with abdominal palpation &urine MCS
Note Hypertrophied bladder neck and dilated posterior urethra proximal to valve narrowing.
Anteroposterior view of the abdomen during a void cystourethrographic study. This image demonstrates a dilated bladder with trabeculation, diverticula, and massive reflux.
Lateral view of a voiding cystourethrographic study during voiding after catheter removal. The dilated posterior urethra is highly suggestive of a posterior urethral valve, which is seen as the nonopacified line that separates the dilated posterior urethra from the normal-caliber distal urethra.
Ectopic Ureter • Continuous urinarydribbling vs intermittent • Dry when supine with vaginal pooling
Non-Mechanical Obstruction • Non-Obstructed ‘Obstructed’
Prune Belly Syndrome` • Triad of • 1. Weak abdominal muscles • 2 Undescended testes (cryptorchidism) • 3. Urinary tract problems- atonic ureters End Stage Renal Failure • Formerly didn’t survive; Now do with early Surgery to correct abd. muscles
Bladder Extrophy • Bladder is turned "inside out“; Lr portion fails to form correctly • Urethra & genitalia not formed completely (epispadias) • Anus & vagina appear anteriorly displaced • Pelvic bones widely separated –diastasis • Rx: Series of Surgical Operations
Myelomeningocoele • Myelomeningocele- backbone and spinal canal not close before birth. Associated : • 1. Hydrocephalus in 90% • 2. Big bladder- atonic bladder • 3. Anus: Patulous: lack bowel control • 4.Legs Partial or complete paralysis of legs & loss of sensation
5 5
Myelomeningocoele Rx • Parents fully aware BEFORE BIRTH • Surgery to repair defect at an early age • 3.V-P shunt for hydrocephalus • 4.Antibiotics 4 meningitis or UTI • 5.Wheel chair • 6. Bladder catheterization, Rx CRF- DT
15 yr Survey of 45 CRF,PH Anochie I, Eke F.Ped Nephrol 2003;18:692-5
Yearly Incidence ESRF UPTH,Nigeria Red X, Sth Africa EkeF.NigMedPract1992;35:37 EkeF,EkeN:PedNephrol1994;8:383-386 AnochieI,EkeF:PedNephrol2003:18:692-695
Approach to preventing Deterioration in CKD • A: Surgical • In Utero endoscopic valve ablation or vesico-amniotic shunting • Endoscopic resection of valves 2-3 days of birth • Operation should be done by the most experienced. Valvotomy in UCH-OPD. Catheter few hrs post Op • Severe valves may need vesicostomy or ureterostomy; & Bladder augmentation later
Mechanical Obstruction only one Aspect • B: Medical • Immediate catheterizaton-size 3 Foleys fluid & electrolyte Rx • Long term monitoring of renal & bladder function • Dysplastic kidneys, Ureters & Bladder • These not often respond to the mechanical relief of Obstruction
Bladder & Renal Care Vital • Intermittent catheterization by patient or parents often an integral part of Rx • Yearly U/S- continued or recurrent stasis • Counselling re avoidance of UTI & stasis • Yearly U&E & Cr, if renal function normaltests for Renal Osteodystrophy, bone mineral density, DMSA scan etc • Pts have lost their Txpt. Kidney from poor bladder management • Avoid constipation
Bladder sphincter dysfunction Recurrent UTIs Bowel dysfunction V U R Bowel dysfunction is often part of the constellation; (Dysfunctional elimination syndrome)
Aims of CRF Management • feel normal - well • be normal - like your friends - intellectual development - school / other activities • maintain normal growth • preserving normal family functioning • slow progression to ESRF • prepare for ESRF treatment
nutrition fluid and electrolyte balance acid base status renal osteodystrophy infection anaemia growth hypertension preservation of renal function education and preparation social /psychological support CRF Management Points
Renal osteodystrophy Treatment • hydroxylated vitamin D therapy - 1 hydroxycholecalciferol - 1-25dihydroxycholecalciferol • by daily oral administration
Counselling • Surgery NOT A CURE • Long term Follow Up • Clearly told Paediatrician or Nephrol for Life • Urological Follow Up may also be for Life • Counsel against ‘It is not my portion’ • Multidisciplinary Counselling best
U/S Obstetrician PaedUrologist PaedNephrologist Neonatologist PaedNurses Parents
Paed Nephrologist ±Urologist Vascular/Transplant Surgeon Teachers Psychiatrists PlayTherapists Dieticians Social Workers Adult Nephrologist Churches
End Stage Renal Disease in PUV • 100% 90% 45% • 1919 1990 2011
Survival in PUV 25% 60% 1919 90% 1990 2011
QUIZ • On presentation 8days after birth, this patient’s serum creatinine is 500 Umol • The management should be • 1. Urgent peritoneal dialysis • 2.Urgent haemodialysis • 3. Something else
QUIZ • Can a bladder rhbdomyosarcoma cause this anomaly? • What is the likely cause?
QUIZ • True or False • All children with Posterior Urethral valves have Chronic Kidney Disease