Download
1 / 36
360 likes | 369 Views
“The Concept That Narcotics Are a Reasonable Way to Treat Chronic Pain Is Falling Apart…”. Multimodal Analgesia And Chronic Pain. Much more than minimizing post-op pain For chronic and non-chronic pain patients. Avner Dagan MD March 9 2019.

E N D
“The Concept That Narcotics Are a Reasonable Way to Treat Chronic Pain Is Falling Apart…” Multimodal Analgesia And Chronic Pain Much more than minimizing post-op pain For chronic and non-chronic pain patients Avner Dagan MD March 9 2019
Chronic pain often outlives its original causes, worsens over time, and takes on a puzzling life of its own … there is increasing evidence that over time, untreated pain eventually rewrites the central nervous system, causing pathological changes to the brain and spinal cord, and that these in turn cause greater pain. Even more disturbingly, recent evidence suggests that prolonged pain actually damages parts of the brain, including those involved in cognition.~The Pain Chronicles, by Melanie Thernstrom “Basically, mice who had their nerves injured who had narcotics took twice as long to recover as those who didn’t have narcotics. The mechanism behind this was that the narcotics put the cells in the spinal cord into overdrive, causing them to create inflammation.”
Outline • Chronic pain patient and definition • What makes them challenging to treat • What is “standard or traditional” opioid based anesthesia? • What is multimodal anesthesia/analgesia? (just a buzzword?) • What are we trying to prevent? • What are the outcome goals? • PACU goals • Long term goals • What drugs can we use for multimodal anesthesia? • Acetaminophen • Lidocaine infusion • Ketamine infusion • Methadone • Magnesium • Gabapentin, COX2 inhibitors, ketorolac, PO NSAIDS, muscle relaxants • Regional anesthesia (great option if type of surgery permits)
Chronic Pain Patient • Multimodal anesthesia techniques are critically important for chronic pain patients due to their processing of painful stimuli differently than non-chronic pain patients • Hyperalgesia • Allodynia • Stress and psychiatric component/disorder • Neuropathic pain as opposed to visceral pain • Traditional opioid based techniques will not work to make the chronic pain patient comfortable or feel their discomfort is being taken seriously • The large doses of opioids needed to help decrease pain in these patients is dangerous and makes the entire healthcare team uncomfortable • This creates a situation in which the patient does not feel their pain is being adequately addressed and creates significant stress and distrust within the healthcare team • There are real physiologic and health risks with uncontrolled or poorly controlled pain during and after hospitalization • Heart attack • Hypertension and stroke • Lack of ability to participate in PT or even get out of bed for discharge
Chronic Pain Patient • Chronic pain is pain that persists past “normal” healing time or roughly 3-6 months • Affects ~20% of the worlds population • In the USA it affects ~100 million people and cost $600 billion yearly • Chronic pain patients are at significantly increased risk of developing mental illness and mood disorders • In fact, several studies have shown treating depression and anxiety in chronic pain patients dramatically reduces their pain levels • “Overall, recent reviews and meta-analysis support the importance of a broad array of psychosocial factors in shaping pain-related experiences and outcomes across numerous pain conditions.”(Edwards et al., 2016) • E.g., Happiness with job, control over your life, minimal social support, depression
Possible Chronic Pain PathwayThe fear avoidance model of pain (Vlaeyen and Linton, 2000 & 2012)
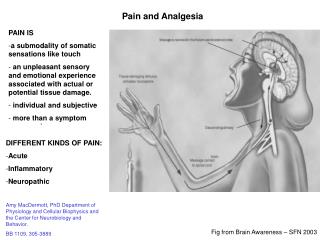
Chronic Pain Mechanisms Peripheral tissue injury causes peripheral inflammation leading to central nervous system inflammation leading to chronic neuronal stimulation/activation leading to chronic pain
Chronic Pain Mechanisms • Surgery causes tissue damage and nerve injury which causes local release of inflammatory biomarkers leading to continual distal nerve activation. • Produces increased nociceptive (free nerve endings) sensitivity causing allodynia and hyperalgesia • Think painful swollen arm after direct injury • Referred to as peripheral sensitization • Prolonged painful stimuli (over the course of a long spine surgery) causes central sensitization in the dorsal horn of the spinal cord • Now you have CNS pain receptors with increased firing to a painful stimulus • Chronically this can lead to changes in the brain leading to decreased descending inhibition of the pain pathways • These are real physiologic changes to the peripheral and central nervous systems caused by tissue injury from surgery or injury • Post-op patient experiences this by increased sensitivity of peripheral nociceptors/lower pain threshold and increased excitability of spinal neurons • Untreated, this can lead to permanent changes in the CNS leading to pathologic chronic pain Key point: remember that narcotics themselves cause central sensitization and chronic pain!
Quick Side-note • When I refer to chronic pain I am mostly talking about surgical injury or accidental injury leading to chronic neuropathic pain • Initial injury or surgical site is completely healed and functional • Patient continues to have significant pain despite “nothing wrong with them” • The other type of patient is someone with ongoing reasons to have significant pain such as cancer or MSK disease etc. • These patients absolutely benefit from multi-modal techniques to minimize the amount of pure opioid they need • However, these patients likely need chronic narcotics, with the goal of reducing total dose Key point: narcotics do not work at all for neuropathic pain, which makes up a huge component of chronic pain. Chronic neuropathic pain uses the glutamate receptor (NMDA) pathway, NOT opioid receptor pathway
Where Does MMA Fit In? • Where can we intervene/target in the peripheral to central sensitization pathway to prevent long term sensitization and prevent or blunt hyperalgesia and chronic neuropathic pain? • We can absolutely intervene during surgery and in PACU to help block intra-op and PACU pain from continuing into central sensitization and causing permanent CNS and brain changes
Key point: narcotics themselves induce central sensitization, hyperalgesia and upregulation of pain receptors in the CNS. Traditional Opioid Based Anesthesia(for chronic and non-chronic pain patients) • Fentanyl administration for induction, tachycardia, hypertension, tachypnea, movement, emergence, analgesia in PACU • Large total dose of short acting opioid • Analgesia gone but CNS effects of narcotic still present • Opioid infusions for neuro or long ortho spine surgeries • Continued opioid administration in PACU and floor/ICU • Summary: • Opioid for any sympathetic disturbance, assumed pain intra-op, post-op • Short lived temporizing opioid administration with very large total dose • Patient may or may not be comfortable in PACU, sedated, delirium, very resistant to further opioid analgesia (not respiratory depression) Descending pain pathways utilize serotonin and norepinephrin; the same neurotransmitters enhanced by antidepressents
What is Multimodal Anesthesia? • “Multimodal analgesia captures the effectiveness of individual agents in optimal dosages that maximize efficacy and attempts to minimize side effects from one analgesic (mainly opioids).” • “Preemptive analgesia involves the introduction of an analgesic regimen before the onset of noxious stimuli, with the goal of preventing sensitization of the nervous system to subsequent stimuli that could amplify pain.” • More effective pain management and less side-effects • The idea being that multiple agents are used that blunt the pain response from different mechanisms of action through both central and peripheral anti-nociceptive modulation • MMA is NOT using a bunch of drugs together to create a sleepy patient in PACU who can not communicate their pain level and then hurts on the floor! • Combination of drugs used are synergistic and significantly reduce need for opioid administration during and after surgery due to a comfortable patient Multimodal Analgesia for Perioperative Pain Management 2011 New Concepts in Acute Pain Therapy: Preemptive Analgesia 2001
Wide Range of Applicability and Benefits • Techniques can be used in conjunction with simple out-patient procedures to very long complex multi-day surgeries • Techniques can be tailored to each patient’s needs and co-morbidities including a history of chronic pain • Patients are discharged from out-patient surgery centers faster, happier with pain control, less PACU OSA complications • Patients avoid remaining intubated after long surgeries, wake up faster, can participate in post-op surgical exams
Goal of Multimodal Anesthesia • Minimize opioid administration intra-op and over total hospital stay • Maximize pain control, physical and mental function peri-op and during hospital stay • Minimize hyperalgesia, CNS sensitization and development of chronic pain • Improve cooperation with PT/OT • Optimize patient pre-op, intra-op and post-op to minimize sedation, confusion, delirium and POCD • Minimize opioid induced respiratory depression and events • Decrease re-admission for severe pain • Happier, comfortable, awake, alert, extubated patient with minimized risk for development of chronic pain, opioid addiction and POCD
Hyperalgesia and Sensitization(what we are trying to avoid) • Hyperalgesia: • Abnormally heightened sensitivity to pain • Can happen after single dose of fentanyl • The more opioid administered the more significant the hyperalgesia • Very high risk with remifentanil • Patients wake up in severe pain minimally responsive to additional opioid administration • Sensitization: (anti-nociceptive and pro-nociceptive pathways) • Upregulation of pro-nociceptive pathways in the dorsal horn of the spinal cord secondary to opioid administration • Opioid administration actually enhances nociceptive pathways potentiating pain and painful stimuli! • Sensitization is not tolerance • Tolerance is decreased response of anti-nociceptive pathways with administration of opioid
Opioid Induced Hyperalgesia(and conversion to chronic pain) • Opioid induced hyperalgesia presents in PACU as an uncomfortable patient who does not respond or minimally responds to opioid administration • Not a theoretical concept. Proven in animal and human studies. • This is the patient who is not responding to “normal” opioid administration doses, hurts more than “usual”, falls asleep then wakes up and hurts, etc.
Overall Short-Term and Long-Term Goals • An awake, alert, respiratory and hemodynamically stable patient who is comfortable • Enhanced analgesia during and after surgery compared to opioid only technique • Avoid hyperalgesia and need for large doses or long term hospital based opioid administration • Minimize risk of opioid induced respiratory complications • Decreased hospital stay • Decreased progression to chronic pain and/or dependence on oral opioids • Decreased risk and/or severity of post-op delirium and POCD • Likely due to decreased opioid administration and less inhaled agent intra-op
Acetaminophen • Question: when and how will you give acetaminophen for maximal benefit? • Acetaminophen works primarily via central mechanisms and must passively diffuse across the BBB to reach “sufficient” CSF concentrations • Acetaminophen’s analgesic and antipyretic affect is directly correlated with its concentration time curve in the CSF • Plasma levels of acetaminophen were correlated with “effective” (pain scores <6/10) analgesia in the PACU. It was found that plasma levels of 10-20 ug/ml were needed to achieve effective pain scores. Singla NK, Parulan C, Samson R, et al. Plasma and cerebrospinal fluid pharmacokinetic parameters after single-dose administration of intravenous, oral or rectal acetaminophen. Pain Pract. 2012; 12:523–532
Acetaminophen Summary • A recent study by B. Crawley et al. (2008) has shown that acetaminophen dosed prior to tissue injury (IT SP) significantly reduces central (spinal) PGE2 concentration and hyperalgesia. • Acetaminophen, if given prior to incision, can dramatically reduce CNS inflammation • Reduces post-op opioid administration by 30% • Strong evidence coming out from Harvard that acetaminophen reduces POCD in the elderly • PO, PR acetaminophen not as effective as IV formulation • Post-op administration still helpful but does not decrease CNS inflammation nearly as much • Strong recommendation to administer IV acetaminophen 1g 30-40 minutes prior to incision, repeat 1g q6 x4 doses • Can be VERY helpful in elderly patients
Lidocaine Infusions • Intraoperative intravenous lidocaine reduces hospital length of stay following open gastrectomy for stomach cancer in men 2012 • Intraoperative systemic infusion of lidocaine reduces postoperative pain after lumbar surgery: a double-blinded, randomized, placebo-controlled clinical trial 2013 • Can intravenous lidocaine decrease postsurgical ileus and shorten hospital stay in elective bowel surgery? 2009 • Low-dose lidocaine reduces secondary hyperalgesia by a central mode of action 2000 • Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery. 2012 • Intravenous lidocaine for post-operative pain relief after hand-assisted laparoscopic colon surgery: a randomized, placebo-controlled clinical trial. 2014 • “Perioperative continuous IV lidocaine infusion has a beneficial effect as regards post-operative pain, restoration of bowel function, and length of hospital stay in patients who have undergone hand-assisted laparoscopic colon surgery.” Pain with movement
Lidocaine Infusion Lidocaine infusions produce pain control well beyond its duration of action
Lidocaine Infusions(real-life benefits) • Patients will have moderately reduced to dramatically reduced pain after surgery with continued reduced pain after lidocaine infusion D/C • Mechanism is thought to be due to reduced central hyperalgesia and blocking of pain signals at afferent nociceptive neurons (blocks Na channels) • Realistically expect a 30-50% reduction in pain scores, narcotic administration and faster wake-ups • There is no definite lidocaine dosing protocol as no one knows the “exact” dose needed • There are over 32 different recommendations for lidocaine infusion dosing • Usual dosing procedure is 1-1.5mg/kg bolus with induction followed by 40mcg/kg/min infusion with maximum dose being 3.5 mg/min • Infusion reaches therapeutic plasma concentration in around 30 minutes • Expect to see significant hemodynamic stability with minimal perturbations in BP and HR and no hypotension • “Train Tracks” • Infusion can be continued until patient leaves OR • Infusion does NOT delay emergence, it enhances smooth emergence • Infusion does NOT cause sedation or alter MS (remember, if there is sedation due to lidocaine your are into toxic levels)
Lidocaine Infusions(Complications and Confusion) • Two most likely scenarios with perceived poor outcomes with lidocaine infusions and PACU: • Patient with significant hemodynamic stability, normal RR intra-op and with extubation causing the provider to not administer any narcotic • Patient starts to hurt in PACU • Perceived outcome is that lidocaine did not do much • How to prevent this? • Provider is unfamiliar with the narcotic sparing effects of lidocaine infusion and administers narcotic based on prior experience • Patient now has the narcotic potentiating effect of lidocaine and high dose narcotic and is slow to wake up in PACU • Perceived outcome is that lidocaine infusions cause delayed emergence and/or simply make patients sleepy • This misconception can be compounded by patient comorbidities and patients who are simply slow to wake up • Remember, lidocaine works on peripheral nerve Na channels and NOT centrally (no sedation, respiratory compromise or hypotension)
Lidocaine Infusions(what it is and what it is not) • A lidocaine infusion will not treat all the patient’s pain (expect 30-50% reduction) • It will not cause sedation in PACU and can be continued at lower dose in PACU (1mg/min) • It will not reach anywhere near toxic levels given in these low dose infusions • Toxicity is simply a non-issue but must still use tele if patient maintained on lidocaine infusion • Used on thousands of patients at UVA, including on floor, with no complications • Do not need to monitor lidocaine plasma levels • If suspect toxicity (normal symptoms of LAST) immediately D/C lidocaine infusion and send lidocaine plasma level • A lidocaine infusion will help achieve and maintain hemodynamic stability and reduce risk of arrhythmias • Will decrease MAC requirement by 30-50% • Reduces inhaled agent requirement, enhancing wake-up • Will decrease central sensitization, hyperalgesia and risk of chronic pain • Will decrease hospital stay and increase patient satisfaction with pain control • Improves bowel motility • Reduces intra-op and post-op narcotic administration and potentiates narcotics that are administered • Will significantly increase SF-12 physical composite scores at 1 and 3 months
Lidocaine Infusions • When to use lidocaine infusions? • The real question is when NOT to use lidocaine infusions! • Can be used in any surgery that may cause pain: outpatient and inpatient • Very useful for outpatient due to narcotic sparing effect, decreased pain with movement • Only relative contraindication to use is severe hepatic dysfunction or confirmed allergy to lidocaine • LidocaineInfusion Summary • Lidocaine infusion is very safe, effective, has multiple benefits that last indefinitely, improves patient outcomes in many areas in addition to pain, very inexpensive and very easy to use and learn • It is simply one component of multi-modal analgesia and is not by itself adequate pain control • Like any drug, it must be fully understood and its effects on MAC, opioid requirements and potentiation studied, evaluated and observed • Provider needs to have realistic expectations of what the lidocaine infusion can and can’t do
Ketamine and Magnesium • Ketamine, and to a lesser extent Mg, bind to and inhibit NMDA receptors in the dorsal horn of the spinal cord • Benefit of ketamine (like lidocaine is multi-factorial) is to inhibit up-regulation of NMDA receptors and substantially reduce CNS sensitization and hyperalgesia pre, intra and post-op. • By blocking and blunting the effect of surgery on the CNS, patients are much more responsive to post-op narcotic administration • Ketamine decreases surgical site pain area, decreases persistent post-operative pain, decreases post-op pain scores and reduces long term pain scores • Administration is a bolus-infusion method with induction • 0.5mg/kg bolus given with induction and an infusion of 2-10 mcg/kg/min • Infusion is terminated 30-40 minutes prior to extubation • Continuation of ketamine infusion will delay emergence • Patient will be asleep but hemodynamically stable and spontaneously breathing
Ketamine and Magnesium • Peri-operative ketamine for acute post-operative pain: a quantitative and qualitative systematic review (Cochrane review) 2005 • Decreased morphine requirement • Decreased PONV • Improved patient satisfaction with pain control • Less pain at 6 months compared to patients who did not receive intra-op ketamine
Ketamine and Magnesium • Key points with ketamine use: • Should be administered as soon after induction as possible • Standard administration protocol is a bolus dose followed by an infusion • Can be given as multiple boluses throughout the surgery • Bolus dose of 20-30mg can be given every 45-60 minutes • Consider avoiding bolus dose if 30 minutes from extubating • Reduce ketamine dose by half if elderly and/or frail patient (use personal judgement) • Ketamine infusion will reduce MAC requirements by 30-50% • In addition to a lidocaine infusion MAC requirement is only, roughly, 30% of normal • Minimal to moderate increase in salivation (especially if prone) • Minimal effect on hemodynamics and will not blunt sympathetic response to surgical stimulation • It may look like ketamine raises BP with administration • Rare psychedelic or emergence delirium from ketamine use • Does not need to be given with a benzo
Ketamine and Magnesium • Common ketamine complications and issues: • Provider unaware of MAC reduction of ketamine and uses “normal” dosing for narcotics and inhaled agent • Patient with delayed emergence in pacu • Provider thinks ketamine is terrible and gets annoyed • Ketamine given close to end of case or too much given intra-op and there is delayed emergence in PACU • Provider thinks ketamine was a bad plan and Avner is trying to sabotage them • Mild confusion in PACU in elderly patients • Still safer than narcotic administration
Ketamine and Magnesium • Ketamine Summary: • Dramatically reduces post-op hyperalgesia, peripheral and central sensitization and post-op pain • Improves pain scores in PACU and months into the future • Minimizes development of chronic pain and drastically reduces wound painful surface area • Synergistic with lidocaine infusions • Profoundly narcotic sparing intra and post-op • Very inexpensive and easy to use
Magnesium • Magnesium is given as a one time bolus after induction • 30-50 mg/kg usually up to 4 gram bolus • Give over a few minutes or may experience transient bradycardia and hypotension • Mg acts as an NMDA receptor antagonist and reduces hyperalgesia and peripheral and central sensitization • Mg also acts as a CCB causing smooth muscle relaxation and muscle spasm reduction (very important in spine surgery) • Strong bronchodilator • Potentiates NDMR and thus if short case make sure patient is fully reversed
Example Surgery • 54 year old 150 kg male in pre-op for T4-sacrum fusion for scoliosis. Patient is otherwise healthy other than 25 year history of chronic pain. Patient is on oxycontin, oxycodone, fentanyl patch, gabapentin, carbamazepine and still has baseline pain of 10/10. • Patient case is delayed 2 hours due to dirty instruments and receives 250 mcg fentanyl, 2 mg hydromorphone but is still in 10/10 pain. • Normal IV GA induction performed and ETT placed • 1 g IV acetaminophen administered • Ketamine bolus given followed by an infusion • Lidocaine infusion started • Patient extubated at end of 14 hour surgery with 0.5 mg hydromorphone given immediately prior to extubation • Patient awake, alert and comfortable in PACU within 15 minutes • No additional narcotics administered in PACU and patient sent to floor with hydromorphone PCA • YES, pain scores checked on floor and all less than 7 • Patient very satisfied with pain control and hospitalization
Primary Goal with M.M.A • Use agents at your disposal that prevent hyperalgesia, sensitization and chronic pain by attacking it with multiple inhibitory mechanisms • Acetaminophen blunts and prevents CNS inflammation and propagation of inappropriate neuronal signaling (especially in the elderly) • Lidocaine blocks Na channels in peripheral nociceptors minimizing CNS bombardment of pain signals and minimizing hyperalgesia, sensitization and progression to chronic pain • Ketamine blocks upregulation of NMDA receptors in the spinal cord and also prevents hyperalgesia, sensitization and progression to chronic pain • Ketorolac and methocarbamol are also very useful adjuncts post-op • Money and Time: • $34 for acetaminophen, $8 for lidocaine, $20 for ketamine • 5 extra minutes to obtain and set up in OR • It is critical to understand that opioid administration during surgery only enhances pain signaling post-operatively. • The less narcotic given during surgery the less the patient needs after surgery