Download
1 / 25
250 likes | 253 Views
This presentation discusses the impact of implementing a process flow tool on reducing wait times for patients admitted to the ICU from the emergency department. The study found that implementing the tool decreased wait times and improved outcomes for critically ill patients.

E N D
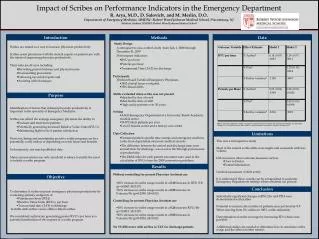
Impact of Process Flow Tool on Wait Times from Emergency Department to ICU Presenter: Pratik Doshi, MD Assistant Professor, Director of Emergency Critical Care Department of Emergency Medicine Division of Critical Care Medicine, Department of Internal Medicine University of Texas Health Science Center, Houston, Texas .
Conflict of interest • None
Overview Chalfin et al. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit care med 2007; 35: 1477-83. ●65,000 Emergency Department visits per year ▪ 37% admitted to hospital ▪ 10% of admitted patients admitted to ICU ● Delayed ICU transfer (>4 hours from care complete to ICU arrival) ▪ Increased hospital mortality ▪ Increased hospital LOS ▪ Increased ICU LOS
Baseline Data March 08- February 09 Care Complete to Depart MICU Admits Mortality 18% higher Length of stay 11% higher
Overview Largest Variation : Care complete to departure
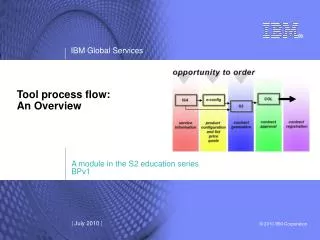
Methods • Prospective case Controlled Trial from 2/2008-9/2010 • In Phase 1:Compare the outcomes of medical ICU admissions between those with ED to ICU wait times < 4 hours with those > 4 hours • In phase2: compare similar outcomes after introducing a qualifying admissions tool designed to reduce wait times to admission • An admission pre-qualifying checklist, standardized nurse documentation, and accelerated bed management process redesign was introduced
Actions Creation of standard operating procedure with an admission algorithm Checklist of contraindications for MICU admission to be filled out on all patients admitted to MICU by EM faculty Standardization of nursing documentation of times of departure Defect log in MICU Educated Faculty, residents, and nursing staff to highlight problems and clarify processes
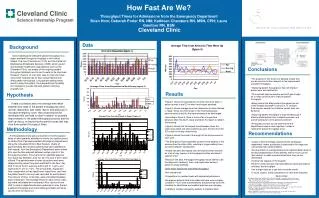
Results Mean time from Emergency room care complete to MICU admission decreased by 2.04 hours(37 %), from 5.53 hours to 3.49 hours
Results Mean time for Emergency department arrival to departure decreased by 1.98 hours(22%) from 8.81 hours to 6.83 hours.
Conclusions • Boarding of critically ill patients in the Emergency department has an association with worse outcomes • Emergency room based process flow tool can be effective in reducing the wait times for patients admitted to the ICU • This decrease in boarding times seems to be associated with decreased hospital length of stay
Conclusions • Mortality rates remained stable • More patients in the lower mortality and LOS group translates into potential lives saved and definite hospital days saved • The hospital days saved total a potential of 990 days, at a rate of 1.54 days for the 643 admissions after the process was instituted, which results in a conservative estimate of $1,039,500 of cost avoidance over the year.
Key Learning No Magic Bullet Walk the process Solution should be the result of process, not pre-conceived Solution may just be “leaning” the process
Team Members Brent King, MD: Chair, Department of Emergency Medicine James McCarthy, MD: Medical Director, Department of Emergency Medicine Bela Patel, MD: Medical Director, Medical ICU Yashwant Chathampally, MD: Department of Emergency Medicine Ruth Siska, RN and Tammy Campos, MSN: Medical ICU Sylvia Reimer, RN and Janice Hughes, RN: Emergency Department Katharine Luther