Download
1 / 57
580 likes | 614 Views
Patient mobility, Range of Motion exercises, Pressure Area Care. Revised and edited March 2012 Michele Archdale References: Tabbner’s Nursing Care 5E 2009. Why is positioning important?. Good posture achieved when the body is in correct alignment

E N D
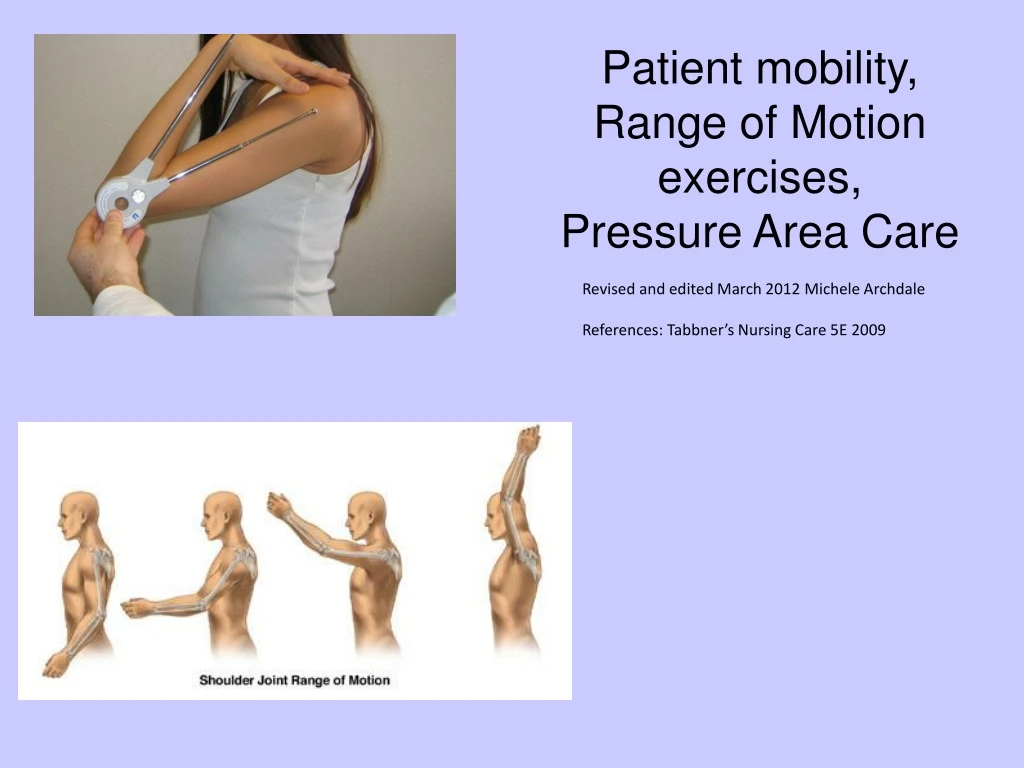
Patient mobility, Range of Motion exercises, Pressure Area Care Revised and edited March 2012 Michele Archdale References: Tabbner’s Nursing Care 5E 2009
Why is positioning important? • Good posture achieved when the body is in correct alignment • Prevent contractures: characterized by flexion & fixation & caused by atrophy & shortening of muscle fibers or by loss of normal elasticity of the skin • Prevent injury / Ulcers Pressure Sores – tissues are compressed, decreased blood supply to area, therefore, decreased oxygen to tissue & cells die. • Stimulate circulation • Promote lung expansion • Relieve pressure and joint tightness • Comfort & pain relief
Moving & Positioning • Mobility – persons ability to move about freely. • Immobility – person unable to move about freely, all body systems at risk for impairment. • It is important to maintain proper body alignment for the patient at all times, this includes when turning or positioning the patient. • Aim – least possible stress on patient’s joints & skin. Maintain body parts in correct alignment so they remain functional and unstressed. • Patients who are immobile need to be repositioned every 2 hrs. (2/24)
Application of proper body mechanics “By applying the nursing process and using the critical thinking approach, the nurse can develop individualized care plans for clients with mobility impairments or risk for immobility. A care plan is designed to improve the client’s functional status, promote self care, maintain psychological well being, and reduce the hazards of immobility.” (Potter and Perry, 2006)
Moving & Positioning: Nursing Process • Assessment • Comfort level & alignment while lying down • Risk factors - Ability to move, paralysis • Level of consciousness • Physical ability/motivation • Presence of tubes, equipment • Wounds • Pain • Nursing Diagnosis • Defining characteristics from the assessment • Activity intolerance • Impaired physical mobility • Impaired skin integrity
Nursing Process (cont.) • Planning • Know expected outcomes – good alignment, increased comfort • Raise bed to comfortable working height • Remove pillows & devices • Obtain extra help if needed • Explain procedure to client • Gather necessary equipment • Multitasking – wash at same time?
Nursing Process (cont.) • Implementation • Offer pain relief as necessary • Consult care plan • Wash hands • Close door/curtain • Put bed in flat position • Move immobile patient up in bed • Realign patient in correct body alignment (pillows etc.)
Nursing Process (cont.) • Evaluation • Assess body alignment, comfort • Ongoing assessment of skin condition • Use of proper body mechanics (nurse)
Tips for positioning the patient • After turning – use aids i.e. pillows, towels, washcloths, blankets, sandbags, footboards etc. • Joints should be slightly flexed b/c prolonged extension creates undue muscle tension & strain • Supine
Types of Positions • Supine (dorsal recumbent) • Prone (anterior recumbent) • Semi-recumbent • lateral • Sim’s • Coma • Dorsal • Lithotomy • Genupectoral (knee-chest) • Orthopnoeic; Dorsal Recumbent
A= supine B= prone C= semi recumbent D= lateral E= Sim’s F= Coma G= Dorsal H= lithotomy I= Genupectoral
SUPINE • Flat on back, pillow under head • Limbs – normal alignment • Pillow if needed to maintain normal position of feet • Relaxation of abdo muscles • Relieves tension on abdo area • Several hours after lumbar puncture to facilitate normal circulation of CSF; helps to prevent severe headache • Low or flat pillow (prevents neck flexion) • Trochanter role (supports hip joint prevents external rotation) • Hand roll – used if hands are paralyzed (thumb & fingers flexed around it) • High top sneakers, foot board, sandbags (support feet with toes pointing upward. Prolonged plantar flexion leads to foot drop (permanent plantar flexion & inability to dorsiflex)
Disadvantages: • Restriction of chest expansion – complications • Difficulty toileting – retention • Loss of independence – depression • Increased work of heart – lying flat increased venous return (preload) • Pressure necrosis of skin • Occipital- may be assessed. • Sacral – pressure sores • Heels – a special & serious risk in diabetic pts • Postoperative backache • Use of a lumbar support may be beneficial
Prone – anterior recumbent • Head supported on small pillow • Lies on abdo- pillow to ensure natural curve of the spine & relieves pressure on breasts • Pillow may be placed under ankles or toes extended over mattress • Comfortable positioning of arms
Use support to protect pressure points, toes and feet as done in this picture.
To relieve pressure on posterior surface of the body – promote healing & relieve pain e.g.burn, ulcer. • Provision of access to posterior surface of body. • Promote drainage from respiratory tract – elevation of foot end of bed?
Disadvantages • Restriction of chest expansion – complications • Loss of independence – depression • Difficulty with ADL’s – eating drinking toileting etc. • Counter indicated with spinal cord problems.
Prone Position 2 Airway, airway, airway!!! Pressure points Ladies’ breasts Men’s genitailia
Semi-recumbent • Lies on back • Three – four pillows supporting head, neck and shoulders • No specific indications – may be comfort only related.
LATERAL • Lies on side head supported with a pillow. • Arms in front of the body – supported with pillows. • Legs flexed or extended. • Pillows along the back and or between knees. • Even if paralyzed on one side a patient can be placed on that side. Take care not to pull on the affected extremity.
Left lateral – examination / treatment invoving rectum. • Lumbar puncture – spine flexed. • Unconscious client – promotes maintenance of clear airway. • Prevents oral secretions entering trachea.
Pressure problems • The skin below the iliac crest is at risk • The underlying deltoid can suffer ‘crush syndrome’ • The underlying sciatic nerve is at risk in emaciated pts • Axillary support is essential to protect the underlying brachial plexus
Sims Position Not used frequently. Can be used for vaginal examination – perhaps less embarrassing. Upper leg drawn towards chest, buttocks towards edge of bed. Lower arm placed behind client. Upper arm in front. Pressure points are different from other positions, i.e. supine, thereby preserving skin integrity.
Coma • Basically Sim’s position but without a pillow under the head. • Correct positioning of head essential for clear airway – pillow may impede breathing. • Temporary position during unconsciousness – e.g fainting. • Prevents tongue / oral secretions from obstructing trachea.
Disadvantages – prolonged use • Restriction of chest expansion – complications • Postural deformities – contractures • Prolonged pressure on arm & shoulder placed behind client– damage to brachial plexus.
Dorsal • Lies on back – knees flexed and apart. • Soles of feet flat on bed. • Head supported by a pillow. • Indications: • Insertion of urinary catheter. • Vaginal examination • Enema / rectal suppositories if unable to assume left lateral position.
Variation to dorsal – lithotomy • Gynaecological exam • Birthing • Disadvantages • Embarrassing • Nervous system complication • Straight leg sling system may cause nerve problems • Compartment syndrome - This can result from undue pressure on the calf muscles • Increased intra-abdominal pressure enhances the possibility of gastric regurgitation
Genupectoral • Knee – chest, client kneeling • Indications: • Specific examination of lower colon to facilitate insertion of instruments. • Management of specific obstetric emergencies. • Disadvantages: • Uncomfortable • Embarrassing • Difficult to maintain • Could result in dizziness, fainting and falling.
There are three variations of a sitting position: • The semi-upright, or semi-Fowler's, position, in which the client sits at an angle of about 30 degrees, supported by pillows, which are placed against the backrest of the bed • The upright, or Fowler's, position, in which the client is in a full sitting position, with pillows placed to support the upper body • The orthopnoeic position, in which, from an upright position, the individual leans onto an over-bed table
A particular one of these sitting positions may be indicated: • After abdominal or thoracic surgery. Less tension is exerted on an abdominal wound, therefore comfort is promoted. Drainage by gravity from body cavities is facilitated (e.g. when there has been a drainage tube inserted after surgery) • To facilitate breathing and reduce dyspnoea. Because the diaphragm is able to flatten, maximal chest expansion is promoted and the risk of lung congestion is decreased. Leaning forward, as in the orthopnoeic position, helps to increase lung capacity and therefore alleviate distressed breathing • To facilitate independence, as a sitting position enables the client to see and participate in ward activities. The activities of daily living (e.g. eating and drinking or using toilet utensils) are also facilitated in this position. • The disadvantages of a sitting position include: • Difficulty maintaining the position, which may become tiring or uncomfortable • Difficulty in sleeping • Prolonged pressure on the buttocks and sacral area, which increases the risk of decubitus ulcers • Difficulty maintaining a comfortable body temperature: in cold weather it may be hard to bring the bedclothes up to the shoulders, while in hot weather the client may experience discomfort from the number of pillows required to maintain a sitting position.
In the Trendelenburg position the body is laid flat on the back with the feet higher than the head by 15-30 degrees, in contrast to the reverse Trendelenburg position, where the body is tilted in the opposite direction. • This is a standard position used in abdominal and gynaecological surgery. It allows better access to the pelvic organs as gravity pulls the intestines away from the pelvis.
Clients in Bed Evaluate Comfort After Positioning for Alignment Check for tubes, equipment, bed creases Reposition 2hrly Use Repositioning for effective ROM Use Supportive Devises for Positioning
Patient mobility • Encourage independence at all times • Assess client • Physio input? • Attitudes play a part – socio-economic status, upbringing • Provide information & support • Functional decline associated with disuse. • Being fit makes it easier to perform daily activities & improves recovery after illness. • Prevalence of obesity – current trends 1 in 3 obese • Obesity – leads to severe health problems • Nurses role in education and encouragement.
Types of Range of Motion • Nurses may need to assist and encourage ROM exercise when activity is limited. • Active Range Of Motion • Passive Range Of Motion • Active Assistive Range of Motion (We assist patient) • ROM is the extent of movement that a joint is normally capable of.
ROM Goals To keep patient in the best physical shape possible. To increase joint mobility. To increase circulation to the affected part.
Assessing Joint Mobility The ROM is appropriate to each joint.
Precautions with ROM • Infection or inflammation around a joint. • Pain • Osteoporosis • Arthritis
Limitations Swelling, tenderness & pain are among factors that limit ROM.
Passive ROM The patient is unable to move independently and someone else manipulates body parts.
Active-Assistive ROM The nurse provides minimal support as the patient moves through ROM.
Active ROM The patient moves independently through a full ROM for each joint.
Hip ROM Hip ROM includes flexion, extension and lateral & external rotation Adduction & Abduction
Hand Movements (ROM) ROM in wrist includes flexion, extension. ROM in hands include abduction, adduction, flexion, extension, opposition and circumduction of the thumb.
Restraints • Device used to immobilize a client or an extremity • A temporary means to control behavior • Restraints are used to: • Prevent falls & wandering • Protect from self-injury (pulling out tubes) • Prevent violence toward others • Restraints deprive a fundamental right to control your own body. • While restraint-free care is ideal, there are times that restraints become necessary to protect the patient & others from harm. • Highly agitated, violent individual – Physical/Chemical restraints • Intubated patient – pulling out endotracheal tube • Suicide patient - ? Chemical restraints
Goals of Restraint Use • To avoid the use of restraints whenever possible. • Encourage alternatives • Family member to sit with patient • Geri chair vs. bed • Consider restraints as a temporary measure – decrease likelihood of injury from restraint use. • Remove restraints as soon as the patient is no longer at risk for injury. • Trial periods of removal of restraint.