Download

1 / 92
1k likes | 1.44k Views
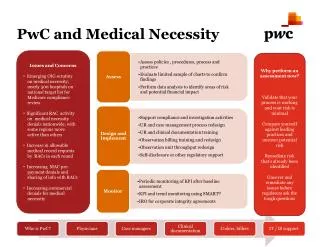
Medical Necessity. Concept in Practice. Medical Necessity: Who Cares?. What payers? What about accreditors? Even for rehab option? What about recovery programs and services ? Isn’t this something only the doctor can determine? What about client choice?. Medical Necessity: Who Cares?.

E N D
Medical Necessity Concept in Practice Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • What payers? • What about accreditors? • Even for rehab option? • What about recovery programs and services? • Isn’t this something only the doctor can determine? • What about client choice? Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • PAYERS • Medicaid • Medicare • Champus/Tricare • ODMH • ODADAS • Commercial insurers Mary Thornton & Associates, Inc
OIG’s Red Book 2002 Red Book once again cites MH: “the IG found that Medicare could save $685 million by reducing claims error rates for mental health services. (Error) Rates exceeded 34% suggesting numerous and widespread problems. The IG suggested CMS monitor cases of under-utilization, over-utilization, medical necessity and reasonableness.” Mary Thornton & Associates, Inc
OIG Audit of Medicare Part B Outpatient MH Services • May 2001 Release • Review of core services, not partial hospital • Review of 1998 services: $1.2 billion spent on mental health by Medicare –60% is outpatient • Over half of services audited were to beneficiaries who are eligible because of disability, not age Mary Thornton & Associates, Inc
OIG Audit of Medicare Part B Outpatient MH Services • 34% of individual therapy services inappropriate • 50% of group therapy services inappropriate • 40% of psych testing services inappropriate • 16% of pharmacological services inappropriate Mary Thornton & Associates, Inc
OIG Audit of Medicare Part B Outpatient MH Services • 41% billed inaccurately: wrong code, non-covered services, excessive billing • 11% unqualified providers • 65% poor documentation • 23% medically unnecessary • 22% receiving more services than necessary • 8% not receiving enough services Mary Thornton & Associates, Inc
GAO Testimony on Medicaid Fraud (Nov 1999) • Three primary categories of fraud and abuse: • Improper billing practices: upcoding, phantom TX, delivering more treatment than is necessary • Misrepresenting qualifications: false credentials, performing outside the bounds of one’s license • Improper business practices: kickbacks for referrals to a provider or product, anti-trust, cost reports issues, enhancement of profits by limiting care Mary Thornton & Associates, Inc
GAO and Medicaid • This year for first time GAO adds Medicaid to list of programs at High Risk for fraud and abuse • Cites schemes by states to leverage funds • Waiver programs that increase costs • Insufficient oversight to assure providers paid appropriately Mary Thornton & Associates, Inc
GAO and Medicaid • January 30, 2003 Report • Argues for more and more aggressive state Medicaid anti-fraud initiatives • States are not collecting all they could for fraud efforts from feds because they would have to match - .01% being spent on payment safeguards • Efforts to identify improper payments limited and modest in scope Mary Thornton & Associates, Inc
The OIG’s Work Plan: Other Medicaid Services • Waiver Programs • Cost neutrality and costs effectiveness of Medicaid waiver programs being questioned • 2 years ago Home and Community Based Waiver programs for the Mentally Retarded were cited Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • What about accreditors? • Medical necessity is a payment concept • Medical necessity and quality of care are linked • Treatment should be the least restrictive, considering the safety of the client and their current status (signs, symptoms, functioning) Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • Even for rehab option? • Rehab option services are either paid for by Medicaid or by state funds that follow the Medicaid model • Medical necessity is a foundation concept Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • What about recovery programs and services? • Many services that are critical to a recovery-based model of care are being paid for through the rehab option, e.g. skill building, psychosocial rehab, residential support, and others • Some recovery-focused services such as peer support and most recreational services are not paid for under rehab option and payment is not based on medical necessity Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • Isn’t this something only a doctor can determine? • No • Diagnosing professionals • Treatment planning signers • Managers of care • Once initial case made, continuing confirmation is found in progress notes and other documentation – the entire treatment team participates Mary Thornton & Associates, Inc
Medical Necessity: Who Cares? • What about client choice? • They can choose to receive services that are not medically necessary • Those services must be paid for by the client or by alternate available resources • Billing for non-medically necessary services is a problem • Paybacks • Potential for investigations, fines, etc. Mary Thornton & Associates, Inc
Productivity and Medical Necessity Mary Thornton & Associates, Inc
Medical Necessity: What’s it mean? Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Starts with a qualified professional • Assessment • Clinical Formulation • Diagnosis • Determination of level of care • Ordering treatment • Scope of license issues Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Services ordered are necessary for Dx or Tx of disease, illness, or injury and without which the patient can be expected to suffer prolonged, increased or new morbidity, impairment of function, dysfunction of a body organ or part, or significant pain and discomfort.”1 1Ohio Adminstrative Code, 5101:3-1-01 Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Deconstructing Medical Necessity: • “Services ordered are necessary for diagnosis” • Initial assessments are usually covered unless internal transfer • Reassessments should be done only if there is a need to update information • E.g. Medicare pays for an assessment every three years or after any changes to level of care • Psych testing should be done for diagnostic purposes only and then only if additional information is needed that cannot be obtained from an interview • Consultations and other diagnostic work – e.g. labs, etc. may be covered in order to diagnose. Need clear link. 1 Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Deconstructing Medical Necessity: • Services ordered are necessary for treatment of disease, illness, or injury • Client must have a reimbursable diagnosis • Mental health vs substance abuse • DSM vs. ICD-9 • Axis III/Medical Conditions important: • Comorbidities may create additional complexity • Mental retardation: limits mental health services • Alzheimers and other forms of dementia • Deafness and other communication problems Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Deconstructing Medical Necessity: • “without which the patient can be expected to suffer prolonged, increased or new morbidity, impairment of function, dysfunction of a body organ or part, or significant pain and discomfort.” • Treatment can be focused on preventing backsliding • Treatment can be focused on impairment of function • Treatment can be focused on prevention of new morbidities, Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Medically necessary services are those that: • Are not experimental and are generally accepted as effective for the problem being addressed • Delivered at an appropriate intensity • Provided at the appropriate level of care setting • When used for diagnosing capable of providing “unique, essential and appropriate information” Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Medically necessary services are those that: • Are not experimental and are generally accepted as effective for the problem being addressed • Watch inappropriate psychotherapy Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Medically necessary services are those that: • Delivered at an appropriate intensity • Be concerned with too little and too much • Meds only clients • Frequent no shows • Non-compliance Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Medically necessary services are those that: • Provided at the appropriate level of care setting • Do you have written levels of care that are accessible, well distributed, and being appropriately used by staff? • Be concerned with appropriate and timely transfers and discharges • Be also concerned with non-compliance with appropriate levels of care – good documentation to describe attempts to move clients Mary Thornton & Associates, Inc
Medical Necessity: What’s It Mean? • Ohio Medicaid: • Medically necessary services are those that: • When used for diagnosing capable of providing “unique, essential and appropriate information” • Additional diagnostic tests must be capable of providing information that is not available in other, less expensive ways. Mary Thornton & Associates, Inc
Criteria for Payment • In addition to tests of medical necessity, Ohio Medicaid is looking for additional information before agreeing to pay • Services must be voluntary and initiated by client • Evidence of client choice of provider • Eligible providers must render service • Compliance with definition of service • Service must be lowest cost service that effectively addresses client’s problem Mary Thornton & Associates, Inc
Additional Guidance for MH and SA • DSM IV or ICD 9 CM diagnosis • Client must be active participant • Sufficient cognitive ability to benefit • Services must be: • Provided according to an individualized service plan • Least restrictive setting that is available and safe • Developmentally appropriate for children Mary Thornton & Associates, Inc
Additional Guidance for MH and SA • DSM IV or ICD 9 CM diagnosis • Dx alone is not enough • Dx + Signs/Symptoms • Dx + Functional Status • Dx + Signs/Symptoms and Functional Status • Current signs/symptoms and functional status is critical to medical necessity • Acuity/other clinical information in 5th digit of ICD 9 • Each service must be directed toward an appropriate diagnosis Mary Thornton & Associates, Inc
Additional Guidance for MH and SA • Client must be active participant • Documentation must be clear about client’s participation in treatment • Besides being present- what else? • Non-compliance • Catatonia and other diagnoses that may prevent participation • Watch billing for these • Signing treatment plans, progress notes Mary Thornton & Associates, Inc
Additional Guidance for MH and SA • Sufficient cognitive ability to benefit • Watch for: • Very young children • Dementia – all kinds – fight if you think it is appropriate at early stages of disease • Mental retardation – except for mild and sometimes moderate • Autism • Other clients who cannot benefit – e.g. intoxicated Mary Thornton & Associates, Inc
Additional Guidance for MH and SA • Services must be: • Provided according to an individualized service plan • Every service must be ordered • Least restrictive setting that is available and safe • Please note available • Rehabilitation option services must be considered. • Developmentally appropriate for children Mary Thornton & Associates, Inc
Rehabilitation Option • Federal Definition: • “Any medical or remedial services (provided in facility, home or other settings) recommended by a physician or other licensed practitioner of the healing arts, within the scope of their practice under state law, for the maximum reduction of physical or mental disability and restoration of the individual to the best possible functional level.” Mary Thornton & Associates, Inc
Rehabilitation Option IAPSRS Definition of Rehabilitation Model: • “Focuses on the functioning of the individual in the normal, day to day environment, and looks at the strengths and skills people bring to the rehabilitation process and supports in the community. “ Mary Thornton & Associates, Inc
Rehabilitation Option IAPSRS Definition of Rehabilitation Model continued: • “Although an individual may still be symptomatic, the rehabilitation process helps a person learn ways to compensate for the effects of the mental illness thorough environmental supports and coping skills. The person with the mental illness becomes the the expert in managing the disability.” Mary Thornton & Associates, Inc
Why is Rehab Option so important to the payer? • Research has demonstrated that rehabilitation leads to: • shorter hospitalizations • improved social functioning • greater satisfaction • higher productivity and integration in community Mary Thornton & Associates, Inc
Rehabilitation Option Services • Specifically referenced as rehab option covered services in Ohio: • Basic/Daily Skills training • Social Skills training • Residential services • Employment related services • Social/Recreational services • Family Education Services Mary Thornton & Associates, Inc
Rehabilitation Option Services • Social/Recreational – Medical Necessity Criteria still very clear • “Services may not be for the exclusive purpose of social or recreational activity but must evidence a clear therapeutic objective specifically identified in the individual’s service plan….” Mary Thornton & Associates, Inc
Rehab Option Model Community Support Services: Restoration of basic or daily living skills Restoration of social or personal skills Residential Support Illness Management Others: Pre-voc/ed Medication and Somatic Treatment Individual and Group Psychotherapy Other Acute Services: ACT, Partial Hospital, IOP Peer, Recreational, Employment, Vocational Mary Thornton & Associates, Inc
Documenting Medical Necessity • Documentation: Primary means or determining whether claims should be paid. • Making the case for current and for on-going medical necessity: • Assessment; • Treatment plans; • Progress notes; and, • Related lab and other diagnostic work Mary Thornton & Associates, Inc
$4.2 mm payback in cash and services Management did not act to promote integrity, efficiency and accountability Billed for ineligible clients ( did not meet GAF requirement) Destroyed audit trail by shredding service tickets. Florida Outpatient Center Mary Thornton & Associates, Inc
Physicians did not always sign treatment plans Physicians did not always participate in development of treatment plans or their review Tx plans incomplete, sometimes not there at all, or no signature or date of signature Geriatric Day Tx usually had no prior certification Florida Outpatient Center Mary Thornton & Associates, Inc
No evidence of efforts to reduce level of care based on impact of Tx Tx Plans reflected maximum allowable under Medicaid not goals and needs of patients Interns and other students billed w/out sufficient or evidence of supervision Dual billing of Medicaid and contracts Florida Outpatient Center Mary Thornton & Associates, Inc
Documenting the Medical Necessity of Rehabilitation • Service focus is on teaching not providing – cueing, reminding, training, overcoming barriers • “Medical necessity” based on functional criteria. • Community Support is not case management Mary Thornton & Associates, Inc
Documenting the Recovery Philosophy • Consumer choice: treatment planning • Empowerment: focus on strengths based skills development • Non-coercion and self-determination: engaging the consumer in their own recovery • Protection of rights: privacy, choice, complain, to choose their provider, and so forth • Responsibility for managing one’s own health: treatment planning, provider choice, skills and resource development Mary Thornton & Associates, Inc
Rehabilitation Services • Skills development for restoration to maximum functional state • Organized approach to development of new or redevelopment of old competencies • Can use curriculum in community support too • Implies that a baseline has been established • Not clinically focused although clinical services may play an integral or supportive role in treatment • Symptom reduction is not the focus – symptom and disability management is Mary Thornton & Associates, Inc
Rehabilitation Services - Examples • Basic Skills: • Food planning and preparation • Maintenance of living environment • Community awareness and mobility skills • Economic issues: bill paying, budgeting, etc. • Personal hygiene • Medication self-administration Mary Thornton & Associates, Inc
Rehabilitation Services - Examples • Social Skills: • Those necessary for working, getting along with neighbors and landlords, social contacts and development of social network • Problem solving, conflict resolution • Management of stress • Relationship building Mary Thornton & Associates, Inc