Download
1 / 48
490 likes | 632 Views
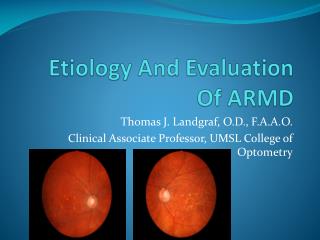
Kevin Colleaux, MD, FRCSC Associate Clinical Professor University of Saskatchewan. ARMD Update 2007. Age-related Macular Degeneration. Incurable, degenerative disease of the macula Leading cause of blindness in adults >55 years. Normal retina. Early AMD. Late AMD retina.

E N D
Kevin Colleaux, MD, FRCSC Associate Clinical Professor University of Saskatchewan ARMD Update 2007
Age-related Macular Degeneration • Incurable, degenerative disease of the macula • Leading cause of blindness in adults >55 years Normal retina Early AMD Late AMD retina Neovascularization Atrophy
Impact Of Age-related Macular Degeneration 0.69 Moderate stroke (requiring help) 0.68 Moderate AMD: 20/50 to 20/100 Ulcerative colitis requiring surgery 0.58 Permanent renal dialysis 0.56 0.47 Severe AMD: 20/200 or worse Severe stroke (bedridden) 0.34 0.0 0.1 0.2 0.3 0.4 0.5 0.7 0.8 0.9 1.0 0.6 Utility score (Patient-reported) Brown GC et al. Trans Am Ophthalmol Soc 2005;103:173–84.
Age & Age-related Macular Degeneration Klein R et al. Ophthalmology 1992;99:933-943; Beaver Dam 1988
Reducing The Risk Of Developing Age-related Macular Degeneration
Uncontrollable Risk Factors • Age • Family history • Gender - female • Race • Iris color
Controllable Risk Factors • Diet • Smoking • Ultraviolet exposure • Excessive weight/obesity • Hypertension
Age Related Eye Disease Study (AREDS) • Demonstrated about 25% reduction in AMD progression with supplements: • Vit E 400 IU • Vit C 500 mg • Beta Carotene 25000 IU • Zinc 80 mg • (copper 2 mg)
Carotenoids • A subclass of xanthophylls • Yellow, oxygen-containing pigments found in plants • Dietary sources: • Spinach, collard greens, broccoli, carrots, corn, citrus fruit • Two major eye nutrients: • Lutein • Zeaxanthin
Managing Exudative AMD in 2007 • A brief history…. • Pre – 2000 • thermal laser • Vision benefit only for extrafoveal discreet lesions • 50% recurrence rate • Most cases untreatable • Treated subfoveal disease universally < 20/200 • 2000 – 2005 • PDT era • 2005 – present • Anti VEGF era
Visudyne Photodynamic Therapy (PDT) • Intravenous infusion of a photosensitive agent (verteporphin) • Laser photoactivation of drug in subretinal tissue • induces thrombosis of neovascular tissue
PDT • Slowed rate of vision loss • Modified treatment parameters and combination with kenalog reduced retreatment and possibly improves outcomes
The Anti VEGF Era • VEGF – Vascular endothelial growth factor • A potent mediator of neovascular growth • Dramatically increases vascular permeability • ‘vascular permeability factor’ • Key factor in exudative ARMD, retinal vascular disease (diabetic retinopathy), and iris neovascularization • Important in maintenance of systemic vascularity and reperfusion, wound healing
Pan VEGF vs Selective VEGF blockade • 5 major isoforms of VEGF • VEGF 165 felt to be the key isoform in ocular neovascular disease • Pegaptamib sodium (macugen) selectively inhibits VEGF 165 • Theoretically should effectively treat ocular disease with lower systemic side effects • Lucentis (ranabizumab) and Avastin (bevacizumab) block all isoforms • ‘Pan VEGF blockade’
MacugenEOP1003, 1004 Combined analysis Weeks after study enrolment Mean change in VA from baseline (number of letters) *Data points estimated from reference Gragoudas ES, Adamis AP, Cunningham ET, et al. N Engl J Med. 2004; 351: 2805–16
Macugen PDT Macugen vs PDT
Vision improvement as the new standard of care in neovascular AMD
Ranibizumab (Lucentis*) (E. coli vector to mass produce) Ranibizumab: Developed Specifically For Ocular Use (AMD) 0 Anti-VEGF-AMurine MAb rhu Fab v1 Affinitymaturation (140x) Humanization Ferrara et al, RETINA 2006; vol 26(8): 859 Data on file (Ferrara)
Lucentis (ranibizumab) vs Avastin (bevacizumab) • Identical mode of action • Efficacy should be similar • Avastin • Off – label use • Hundreds of presentations and publications over past 4 years showing efficacy and safety • Case series and reports, NOT prospective randomized trials • Comparative head to head study currently enrolling at NIH. • Full antibody • Longer half life – increased systemic effect ? • Possibly pro-inflammatory • Lucentis • The gold standard, best data proving efficacy
MARINA treatment schema Month 12 0 1 2 3 4 5 6 7 8 9 10 11 23 24 Ranibizumab0.5 mg Ranibizumab0.3 mg Sham Verteporfin at investigator discretion if: • Conversion to predominantly classic CNV, or • Loss of ≥20 letters on 2 consecutive visits and small (≤4 DA), minimally classicor occult with no classic lesions, with presumed recent disease progression Primaryendpoint prior to Rx Finalvisit Rosenfeld et al, N Engl J Med 2006; 355: 1419
Secondary endpoint:Patients gaining ≥15 letters from baseline Patients gaining ≥15 letters from baseline (%) 100 *** *** *** 34 33 *** 26 25 5 4 0 n=238 238 240 n=189 209 215 Month 12 Month 24 Sham(n=238) Ranibizumab 0.3 mg(n=238) Ranibizumab 0.5 mg(n=240) ***p<0.001 vs sham Rosenfeld et al, N Engl J Med 2006; 355: 1419
Ranibizumab 0.3 mg (n=238) ETDRS letters 10 +7.2 +6.6 +5.4 5 +6.5 21.5 letter difference*** 0 2 4 6 8 10 12 14 16 18 20 22 24 -5 20.3 letter difference*** -10.4 -10 -15 -14.9 Month Secondary endpoint:Mean change in VA over time Sham (n=238) Ranibizumab 0.5 mg (n=240) ***p<0.001 vs sham Rosenfeld et al, N Engl J Med 2006; 355: 1419
Secondary endpoint:Patients with 20 / 200 or worse Patients (%) 100 48 43 *** *** *** *** 15 15 15 13 13 12 12 0 Baseline Month 12 Month 24 Sham(n=238) Ranibizumab 0.3 mg(n=238) Ranibizumab 0.5 mg(n=240) ***p<0.001 vs sham Rosenfeld et al, N Engl J Med 2006; 355: 1419
MARINA 24 monthsSecondary endpoint:Patients with 20 / 40 or better Patients (%) 100 *** *** *** 42 40 *** 39 35 15 15 11 11 6 0 Baseline Month 12 Month 24 Sham(n=238) Ranibizumab 0.3 mg(n=238) Ranibizumab 0.5 mg(n=240) ***p<0.001 vs sham Rosenfeld et al, N Engl J Med 2006; 355: 1419
Summary: MARINA year 2 results • Ranibizumab 0.5 mg patients had a +6.6 letter improvement in visual acuity • 33% of ranibizumab 0.5 mg patients improved ≥15 letters vs 4% of sham patients • 90% of ranibizumab patients lost fewer than 15 letters vs 53% in sham arm Rosenfeld et al, N Engl J Med 2006; 355: 1419
ANCHOR treatment schema Ranibizumab 0.3 mg Ranibizumab 0.5 mg Sham injection Verteporfin Sham PDT 12 Month 0 1 2 3 4 5 6 7 23 24 8 9 10 11 Ranibizumab 0.3 mg Ranibizumab 0.5 mg Verteporfin Sham Primary endpoint Final visit Brown et al, N Engl J Med 2006; 355: 1432
Primary endpoint:Patients losing <15 letters from baseline Patients (%) *** *** 96.4 94.3 100 64.3 0 Month 12 Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=139) Brown et al, N Engl J Med 2006; 355: 1432 ***p<0.001 vs verteporfin
Secondary endpoint:Patients gaining ≥15 letters from baseline Patients (%) 100 *** *** 40 36 6 0 Month 12 Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=139) Brown et al, N Engl J Med 2006; 355: 1432 ***p<0.001 vs verteporfin
Secondary endpoint:Mean change in VA over time Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=139) ETDRS letters 15 +11.3 10 +8.5 20.8 letter difference*** 5 0 18 letter difference*** 2 4 6 8 10 12 -5 -9.5 -10 -15 -20 Month ***p<0.001 vs verteporfin Brown et al, N Engl J Med 2006; 355: 1432
Secondary endpoint:Patients with VA 20 / 200 or worse Patients (%) 100 60 32 *** 25 *** 23 22 16 0 Baseline Month 12 Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=140) ***p<0.001 vs verteporfin Brown et al, N Engl J Med 2006; 355: 1432
Exploratory endpoint:Maintaining baseline VA or gaining ≥0 letters Patients (%) 100 *** *** 77 74 30 0 Month 12 Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=140) Data on file (ANCHOR 12 months) ***p<0.001 vs verteporfin
ANCHOR 12 monthsSecondary endpoint:Patients with VA 20 / 40 or better Patients (%) 100 *** *** 39 31 4 3 1 0 0 Baseline Month 12 Verteporfin (n=143) Ranibizumab 0.3 mg (n=140) Ranibizumab 0.5 mg (n=140) ***p<0.001 vs verteporfin Brown et al, N Engl J Med 2006; 355: 1432
Summary: ANCHOR year 1 results • Ranibizumab 0.5 mg patients had a +11.3 letter improvement in visual acuity • 40% of ranibizumab 0.5 mg patients improved ≥15 letters vs 6% of verteporfin patients • 96.4% of ranibizumab patients lost fewer than 15 letters vs 64.3% in sham arm Brown et al, N Engl J Med 2006; 355: 1432
PIER treatment schema 0 0 1 2 3 4 5 6 7 8 9 10 11 12 23 24 Month Ranibizumab 0.5 mg Sham Primaryendpoint Finalvisit PIER 12 months
10 5 0 -5 -10 -15 PIER:Mean change in VA over 12 months 0 ETDRS letters -0.2 1 2 3 4 5 6 7 8 9 10 11 12 16.1 letterdifference*** -16.3 Month Sham (n=63) Ranibizumab 0.5 mg (n=61) PIER 12 months ***p<0.001 vs sham
Serious ocular safety conclusions 0 • Ocular serious adverse events were not common in ranibizumab-treated patients • <1.5% for each adverse event • Per injection rate of endophthalmitis was <0.1% Rosenfeld et al, N Engl J Med 2006; 355(14): 1419 Brown et al, N Engl J Med 2006; 355(14); 1432
Potential side-effects ofsystemic VEGF inhibition • Arteriothromboembolic events (ATEs) • Assessed using APTC√ criteria • broader scope of event types • Hypertension • Non-ocular hemorrhage • Proteinuria • Other (GI perforation, Impaired wound healing) √Antiplatelet Trialists’ Collaboration, BMJ 1994; 308(6921): 81–106 van Wijngaarden P, JAMA. 2005;293(12):1509-13
Summary of systemic safety • No statistically significant differences in the distribution of ATEs between ranibizumab and control or between the two ranibizumab doses • No higher incidence compared with general AMD population • Patients with cardiovascular history were not excluded from enrollment into ranibizumab studies MARINA and ANCHOR studies
Lucentis (ranibizumab) vs Avastin (bevacizumab) • Identical mode of action • Efficacy and toxicities should be similar • Avastin • Off – label use • Hundreds of presentations and publications over past 4 years showing efficacy and safety • Case series and reports, NOT prospective randomized trials • Comparative head to head study currently enrolling at NIH. • Full antibody • Longer half life – increased systemic effect ? • Possibly pro-inflammatory • Lucentis • The gold standard, best data proving efficacy
Combination therapy • ½ fluence PDT • Plus Avastin / Lucentis • DENALI trial • Plus avastin and dexamethasone • Triple therapy, (Augustin)
Vision improvement as the new standard of care in neovascular AMD