Download
1 / 34
340 likes | 779 Views
THE CELIAC PATIENT. Carol E. Semrad, M.D. Associate Professor of Medicine The University of Chicago. Celiac Disease Sprue Gluten-enteropathy Celiac sprue Inflammatory disease of the small bowel with a known trigger. Same Disease. A Case of “Asymptomatic” Celiac Disease.

E N D
THE CELIAC PATIENT Carol E. Semrad, M.D. Associate Professor of Medicine The University of Chicago
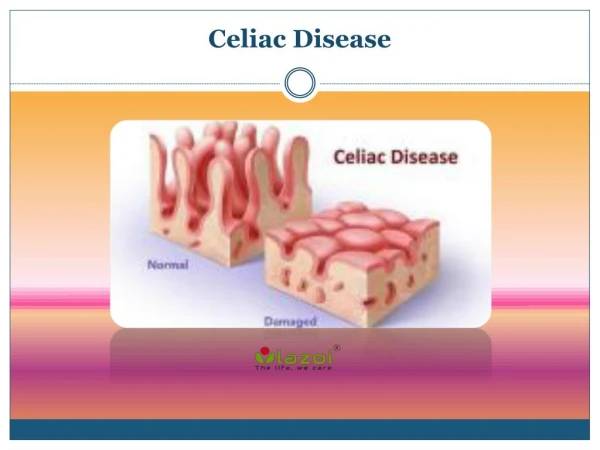
Celiac Disease • Sprue • Gluten-enteropathy • Celiac sprue Inflammatory disease of the small bowel with a known trigger Same Disease
A Case of “Asymptomatic” Celiac Disease • 50 y.o. woman, Italian/Irish • Daughter diagnosed with celiac disease • Screening anti-tTG IgA antibody positive • Occasional indigestion with pasta meals • PMH: Hypothyroidism • FH: Parents of short stature • Physical examination: obese, height 5’1”
Further Studies - Mild anemia, transaminitis, iron deficient - BMD osteopenia • Diagnosis - Celiac disease • Management - Gluten-free diet - Iron therapy - Further evaluation of bone disease - Monitor for improvement
Gluten (the protein component of wheat) Glutenins (alcohol-insoluble fraction) Gliadin (toxic alcohol-soluble fraction) Peptides (33-mer not degraded by human peptidases, contains toxic epitopes) Amino acids (non-toxic to celiac patients)
Celiac Disease GENES • 95% HLA DQ2 heterodimer alleles DQA1*0501 and DQB1*0201(20-30% normals carry these alleles) • 5% HLA DQ8 heterodimer alleles DQA1*0301 and DQB1*0302 • Rarely DQ2 half-heterodimer • Non-HLA genes not yet identified
ADAPTIVE INNATE Intraepithelial CTL NK-like cells ? Lamina Propria Modified from Green and Jabri Lancet. 2003:362;383-91.
Celiac DiseasePrevalence in the U.S.A. • Based on GI symptoms 1:4500 • Based on Antibody studies 1:250 (performed in blood donors) ~ 1% of the Caucasian population
Classical Celiac Disease (1:4500) Atypical Silent Latent Detected by screening (1:250)
Different modes of presentations of celiac disease The clinical presentation of celiac disease is changing Rampertab SD et al., Am J Medicine 2006
Celiac DiseaseClinical Presentation Classical • Diarrhea • Gas/bloating • Weight loss Atypical • Constipation • Dyspepsia • Anemia • Osteoporosis • Rash • Neuropathy/ataxia • Hepatitis • Dental enamel hypoplasia • Infertility • Silent • No sxs/signs • Positive Ab • Abnormal bx • Latent • No sxs/signs • Positive Ab • Normal bx • OR • CD in remission
Celiac Disease Classic, Atypical, Silent Latent Normal Abnormal
Celiac DiseaseDiagnostic Tools Duodenal biopsy Serologies HLA Association anti-tTG IgA, IgGDQ2 A1*05 B1*02 anti-EMA IgA DQ8 A1*03 B1*0302 (anti-DGP)Half DQ2 heterodimer
Antibodies Associated with Celiac Disease IgA Antibody* Sensitivity Specificity MethodAnti-gliadin 57-100% 42-98% ELISA Anti-endomysial 75-98% 96-100% Indirect IF Anti-tissue transglutaminase 98-100% 97-98%# ELISA *False Negative with IgA deficiency #False Positive tTG in IBD, PBC Positive Predictive Value ~ 100% for EMA 80% for human tTG Fasano, Catassi. Gastro2001:120;636 Carroccio et al. Clin Chem 2002:48;1546
CELIAC DISEASE ENDOSCOPY Scalloped Gluten-free diet Normal HISTOLOGY Increased IEL Villous atrophy Recovering
Celiac DiseaseWho Should Undergo Duodenal Biopsy? • High risk with GI symptoms • Dermatitis Herpetiformis • Unexplained iron deficiency anemia • Early osteoporosis/bone fracture • Neuropathy/ataxia • Positive screening antibody test
Celiac DiseaseWho Should Have Antibody Testing? • Support diagnosis • Screening High risk groupsFirst and second degree relatives Dermatitits Herpeteformis Type I Diabetes Mellitus Autoimmune thyroid disease Irritable Bowel Syndrome Primary Biliary Cirrhosis Turner’s and Down’s Syndrome
Celiac diseaseAn approach to antibody screening • tTG IgA antibody and serum IgA level • If positive, confirm with EMA antibody
Celiac DiseaseWhen is HLA Genotyping Helpful? • Family Members -Negative predictive value • Difficulty in securing a diagnosis - Self-started a gluten-free diet - Equivocal small bowel biopsy findings - Positive antibody with normal biopsy - IgA deficiency
Celiac Disease Evaluation • Bone mineral density study - abnormal bone mass in ~ 60% - men > women - if abnormal obtain 25-OH Vit D, PTH, calcium, 24 hour urine calcium • Vitamin/mineral levels in those with evidence of malabsorption/diarrhea - Iron studies and folate - Vitamin A, B12, zinc
Celiac Disease Treatment • Life-long strict gluten-free diet - knowledgeable nutritionist - celiac center web sites/support groups (U. Chicago, Columbia, Mayo Clinic, Stanford, U. Maryland, B.I. Boston) • Oats are tolerated by most • Daily multiple vitamin and calcium • Folic Acid for women of child-bearing age • No initial role for bisphosphonates
Celiac Disease Monitoring • Resolution of symptoms • tTG antibodies for dietary adherence (? correlation between Ab titer and histology) • Weight (risk for obesity) • Cholesterol level • Bone Mineral Density
RESPONSE TO A GLUTEN-FREE DIET 90% IMPROVE 10% FAIL TO IMPROVE(within 2 weeks)Dietary indiscretion Lactose or fructose Intolerance Microscopic colitisWrong Diagnosis Pancreatic Insufficiency Bacterial overgrowth Refractory sprue
Refractory Sprue = Continued symptoms and small bowel atrophy despite a strict gluten-free diet • TYPE I - normal T-lymphocytes population - often responds to steroids, good prognosis • TYPE II -abnormal T cell population (CD3+, CD8-) T-cell receptor-g gene rearrangements - often requires parenteral nutrition - progression to lymphoma - poor prognosis - trials with cytotoxic chemo or stem cell transplant
Celiac Disease Long Term Complications • Anemia • Osteoporosis • Intestinal T-cell lymphoma ? Video capsule endoscopy screening • Other Malignancies Gastrointestinal Melenoma Non-Hodgkins Lymphoma
Celiac DiseaseFuture Treatments • Bacterial Prolyl Endopeptidase • Genetically altered wheat grain • Specific Inhibitors HLA DQ2 tTG IL15 • Tight junction modulators
Summary CELIAC DISEASE • T-cell mediated small bowel mucosa inflammation • Triggered by gluten in the diet in those genetically predisposed • Malabsorption of nutrients • Presents age 2 yrs, young adults, or any age • Diagnosis made by abnormal small bowel biopsy that reverts to normal on a gluten-free diet • Treatment is a life-long strict GF-diet
CELIAC DISEASE Dose-dependent Effect of Gliadin on Small Bowel *capsule of gluten Catassi et al. GUT 1993; 34: 1515 Ciclitira et al. Clin Sci 1984; 66: 357 Catassi et al. Gastroenterol 2005;128:A253
10 mg gliadin ~ 250 mg wheat flour(less than an 1/8 teaspoon flour)
CELIAC DISEASE Are Dietary Oats Tolerated? Janatuinen et al.NEJM 1995;333:1033 Gut 2002; 50: 332 Hogberg et al.Gut 2004;53:649