Download
1 / 1
10 likes | 109 Views
Human Leukocytes Antigen (HLA) Association with Brain Astrocytic Tumors Detected by Genomic DNA Typing. Objectives

E N D
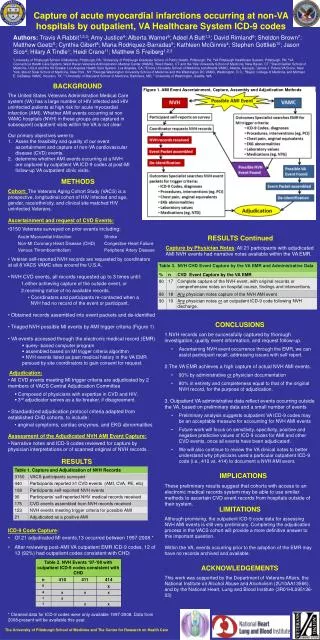
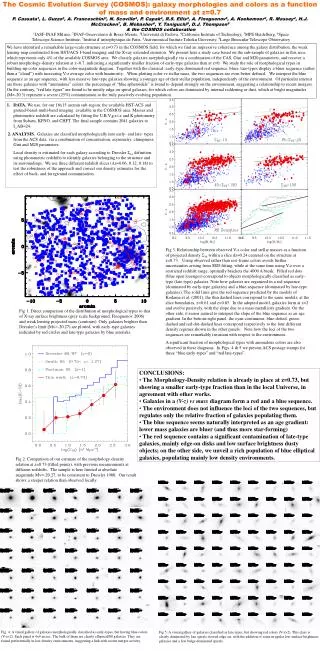
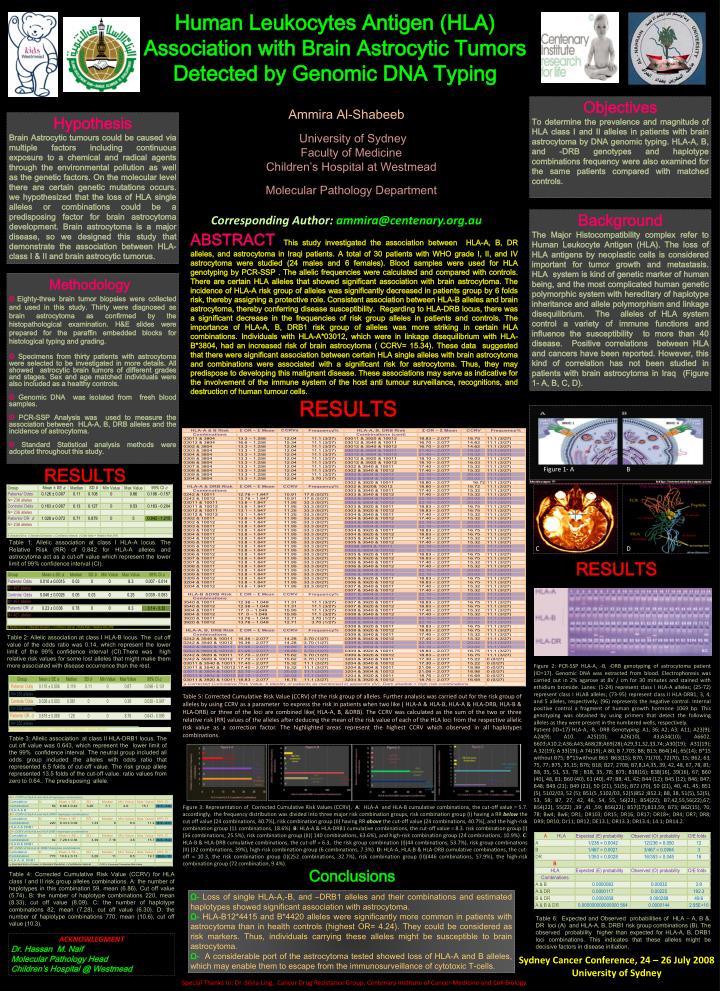
Human Leukocytes Antigen (HLA) Association with Brain Astrocytic Tumors Detected by Genomic DNA Typing Objectives To determine the prevalence and magnitude of HLA class I and II alleles in patients with brain astrocytoma by DNA genomic typing. HLA-A, B, and -DRB genotypes and haplotype combinations frequency were also examined for the same patients compared with matched controls. University of Sydney Faculty of Medicine Children’s Hospital at Westmead Molecular Pathology Department Ammira Al-Shabeeb Hypothesis Brain Astrocytic tumours could be caused via multiple factors including continuous exposure to a chemical and radical agents through the environmental pollution as well as the genetic factors. On the molecular level there are certain genetic mutations occurs. we hypothesized that the loss of HLA single alleles or combinations could be a predisposing factor for brain astrocytoma development. Brain astrocytoma is a major disease, so we designed this study that demonstrate the association between HLA-class I & II and brain astrocytic tumorus. Background The Major Histocompatibility complex refer to Human Leukocyte Antigen (HLA). The loss of HLA antigens by neoplastic cells is considered important for tumor growth and metastasis. HLA system is kind of genetic marker of human being, and the most complicated human genetic polymorphic system with hereditary of haplotype inheritance and allele polymorphism and linkage disequilibrium. The alleles of HLA system control a variety of immune functions and influence the susceptibility to more than 40 disease. Positive correlations between HLA and cancers have been reported. However, this kind of correlation has not been studied in patients with brain astrocytoma in Iraq (Figure 1- A, B, C, D). Corresponding Author: ammira@centenary.org.au ABSTRACT This study investigated the association between HLA-A, B, DR alleles, and astrocytoma in Iraqi patients. A total of 30 patients with WHO grade I, II, and IV astrocytoma were studied (24 males and 6 females). Blood samples were used for HLA genotyping by PCR-SSP . The allelic frequencies were calculated and compared with controls. There are certain HLA alleles that showed significant association with brain astrocytoma. The incidence of HLA-A risk group of alleles was significantly decreased in patients group by 6 folds risk, thereby assigning a protective role. Consistent association between HLA-B alleles and brain astrocytoma, thereby conferring disease susceptibility. Regarding to HLA-DRB locus, there was a significant decrease in the frequencies of risk group alleles in patients and controls. The importance of HLA-A, B, DRB1 risk group of alleles was more striking in certain HLA combinations. Individuals with HLA-A*03012, which were in linkage disequilibrium with HLA-B*3804, had an increased risk of brain astrocytoma ( CCRV= 15.34). These data suggested that there were significant association between certain HLA single alleles with brain astrocytoma and combinations were associated with a significant risk for astrocytoma. Thus, they may predispose to developing this malignant disease. These associations may serve as indicative for the involvement of the immune system of the host anti tumour surveillance, recognitions, and destruction of human tumour cells. Methodology ΘEighty-three brain tumor biopsies were collected and used in this study. Thirty were diagnosed as brain astrocytoma as confirmed by the histopathological examination. H&E slides were prepared for the paraffin embedded blocks for histological typing and grading. ΘSpecimens from thirty patients with astrocytoma were selected to be investigated in more details. All showed astrocytic brain tumors of different grades and stages. Sex and age matched individuals were also included as a healthy controls. ΘGenomic DNA was isolated from fresh blood samples. ΘPCR-SSP Analysis was used to measure the association between HLA-A, B, DRB alleles and the incidence of astrocytoma. ΘStandard Statistical analysis methods were adopted throughout this study. RESULTS RESULTS Figure 1- A B Table 1: Allelic association at class I HLA-A locus. The Relative Risk (RR) of 0.842 for HLA-A alleles and astrocytoma act as a cut-off value which represent the lower limit of 99% confidence interval (CI). C D RESULTS Conclusions Table 2: Allelic association at class I HLA-B locus. The cut off value of the odds ratio was 0.14, which represent the lower limit of the 99% confidence interval (CI).There was high relative risk values for some lost alleles that might make them more associated with disease occurrence than the rest. Figure 2: PCR-SSP HLA-A, -B, -DRB genotyping of astrocytoma patient (ID=17). Genomic DNA was extracted from blood. Electrophoresis was carried out in 2% agarose at 8V / cm for 30 minutes and stained with ethidium bromide. Lanes: (1-24) represent class I HLA-A alleles; (25-72) represent class I HLAB alleles; (73-95) represent class II HLA-DRB1, 3, 4, and 5 alleles, respectively; (96) represents the negative control. Internal positive control a fragment of human growth hormone 1069 bp. This genotyping was obtained by using primers that detect the following alleles as they were present in the numbered wells, respectively. Patient (ID=17) HLA-A, -B, -DRB Genotyping: A1, 36; A2; A3; A11; A23(9); A24(9); A10. A25(10); A26(10), 43;A34(10); A6602, 6603;A10.2;A36;A43;A68(28;A69(28);A29,31,32,33,74;;A30(19); A31(19); A 32(19); A 33(19); A 74(19); A 80; B 7,703; B8; B13; B64(14), 65(14); B*15 without B75; B*15without B63 B63(15); B70, 71(70), 72(70), 15; B62, 63, 75, 77; B75, 35,15; B76; B18; B27, 2708; B7,8,14,35, 39, 42, 48, 67, 78, 81; B8, 35, 51, 53, 78 ; B18, 35, 78; B73; B38(16); B38(16), 39(16), 67; B60 (40), 48, 81; B60 (40), 61 (40), 47; B8, 41, 42; B44 (12); B45 (12); B46; B47; B48; B49 (21); B49 (21), 50 (21), 51(5); B72 (70), 50 (21), 40, 41, 45; B51 (5), 5102/03, 52 (5); B51(5 ,5102/03, 52(5)B52 ;B52.1; B8, 38, 51(5), 52(5), 53, 58; B7, 27, 42, 46, 54, 55, 56(22); B54(22); B7,42,55,56(22),67; B54(22), 55(22) ,39 ,41 ,59; B56(22); B57(17);B13,59; B73; B62(15), 70, 78; Bw4; Bw6; DR1; DR103; DR15; DR16; DR17; DR18+; DR4; DR7; DR8; DR9; DR10; Dr11; DR12; DE13.1; DR13.3; DR13.4; 14.1; DR14.2. Table 5: Corrected Cumulative Risk Value (CCRV) of the risk group of alleles. Further analysis was carried out for the risk group of alleles by using CCRV as a parameter to express the risk in patients when two like ( HLA-A & HLA-B, HLA-A & HLA-DRB, HLA-B & HLA-DRB) or three of the loci are combined like( HLA-A, B, &DRB). The CCRV was calculated as the sum of the two or three relative risk (RR) values of the alleles after deducing the mean of the risk value of each of the HLA loci from the respective allelic risk value as a correction factor. The highlighted areas represent the highest CCRV which observed in all haplotypes combinations. Table 3: Allelic association at class II HLA-DRB1 locus. The cut off value was 0.643, which represent the lower limit of the 99% confidence interval. The neutral group included all odds group included the alleles with odds ratio that represented 6.5 folds of cut-off value. The risk group allele represented 13.5 folds of the cut-off value. ratio values from zero to 0.64.. The predisposing allele. Figure 3: Representation of Corrected Cumulative Risk Values (CCRV), A: HLA-A and HLA-B cumulative combinations, the cut-off value = 5.7. accordingly, the frequency distribution was divided into three major risk combination groups, risk combination group (I) having a RR below the cut off value (24 combinations, 40.7%), risk combination group (II) having RR above the cut-off value (24 combinations, 40.7%), and the high-risk combination group (11 combinations, 18.6%). B: HLA-A & HLA-DRB1 cumulative combinations, the cut-off value = 8.3. risk combination group (I) (56 combinations, 25.5%), risk combination group (II)( 140 combinations, 63.6%), and high-risk combination group (24 combinations, 10.9%). C: HLA-B & HLA-DRB cumulative combinations, the cut-off = 6.3, the risk group combination (I)(44 combinations, 53.7%), risk group combinations (II) (32 combinations, 39%), high-risk combination group (6 combinations, 7.3%). D: HLA-A, HLA-B & HLA-DRB cumulative combinations, the cut-off = 10.3, the risk combination group (I)(252 combinations, 32.7%), risk combination group (II)(446 combinations, 57.9%), the high-risk combination group (72 combination, 9.4%). Table 4: Corrected Cumulative Risk Value (CCRV) for HLA class I and II risk group alleles combinations. A: the number of haplotypes in this combination 59, mean (6.86), Cut off value (5.74). B: the number of haplotype combinations 220, mean (8.33), cut off value (8.09). C: the number of haplotype combinations 82, mean (7.28), cut off value (6.30). D: the number of haplotype combinations 770, mean (10.6), cut off value (10.3). Ω-Loss of single HLA-A,-B, and –DRB1 alleles and their combinations and estimated haplotypes showed significant association with astrocytoma. Ω- HLA-B12*4415 and B*4420 alleles were significantly more common in patients with astrocytoma than in health controls (highest OR= 4.24). They could be considered as risk markers. Thus, individuals carrying these alleles might be susceptible to brain astrocytoma. Ω- A considerable port of the astrocytoma tested showed loss of HLA-A and B alleles, which may enable them to escape from the immunosurveillance of cytotoxic T-cells. Table 6: Expected and Observed probabilities of HLA – A, B &, DR loci (A) and HLA-A, B, DRB1 risk group combinations (B). The observed probability higher than expected for HLA-A, B, DRB1 loci combinations. This indicates that these alleles might be decisive factors in disease initiation. ACKNOWLEGMENT Dr. Hassan M. Naif Molecular Pathology Head Children’s Hospital @ Westmead Sydney Cancer Conference, 24 – 26 July 2008 University of Sydney Special Thanks to: Dr. Silvia Ling, Cancer Drug Resistance Group, Centenary Institute of Cancer Medicine and Cell Biology.