Download
1 / 24
240 likes | 348 Views
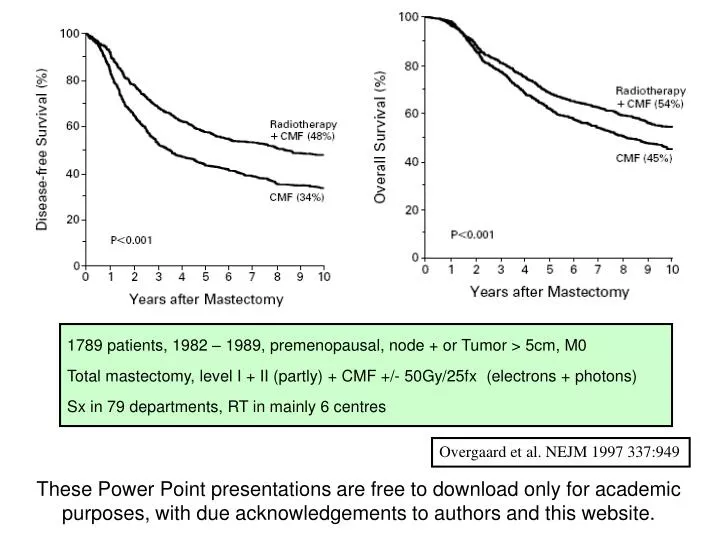
1789 patients, 1982 – 1989, premenopausal, node + or Tumor > 5cm, M0 Total mastectomy, level I + II (partly) + CMF +/- 50Gy/25fx (electrons + photons) Sx in 79 departments, RT in mainly 6 centres. Overgaard et al. NEJM 1997 337:949.

E N D
1789 patients, 1982 – 1989, premenopausal, node + or Tumor > 5cm, M0 Total mastectomy, level I + II (partly) + CMF +/- 50Gy/25fx (electrons + photons) Sx in 79 departments, RT in mainly 6 centres Overgaard et al. NEJM 1997 337:949 These Power Point presentations are free to download only for academic purposes, with due acknowledgements to authors and this website.
64% 56% 318 patients, 1979 – 1986, premenopausal, node +, any T, M0 MRM + CMF +/- 37.5Gy/16fx RT (photons) Sx by ‘specialists’, CT & RT in one centre 54% 41% Ragaz et al. NEJM 1997 337:956
1460 patients, 1982 – 1990, postmenopausal, node +, any T, M0 MRM + Tamoxifen +/- 50Gy/25fx RT (electrons + photons) Sx in 79 departments, RT in mainly 6 centres Overgaard et al. 1999, 353:1641
Vascular deaths: Proportional excess ratio=1.3, absolute rates 3 fold greater
What were the problems with the EBCT review? • Diverse surgical treatments (BCT, MRM, RM, simple mastectomy) • Systemic therapies (including trials with no systemic therapies) • Radiotherapy doses, areas treated, kind of radiation, doses to the heart
Loco-regional failure (LRF) is 25% for >4 nodes; T >5 cm; < 6 nodes at axillary dissection; patient younger than 40 • PMRT reduces this risk to 6 – 8% (absolute benefit of 17-19 women for each 100 treated) • In the subgroup of 1-3 nodes, LRF is 13%; PMRT reduces this to 3-4% (absolute benefit of 9-10 women for every 100 treated) • For a LRF reduction of 20%, cancer specific survival improves by 4-5% • A North-American trial on PMRT for 1-3 nodes was closed due to insufficient interest!!!
Objective: Information and recommendations on PMRT Outcomes: LRC, DFS, OS, toxicities Source of evidence: Review of meta analysis, consensus statements1966 – 2002 + RCTs between 1995 – 2002 (to supplement ASCO guidelines)
Recommendations -1 • PMRT: Tumor > 5cm, invasion of skin, pectoral muscle or chest wall • PMRT: 4 or more positive nodes • PMRT ??: 1-3 positive nodes Danish 82b: T > 5cm : LR failure 12%(RT) vs 42% (no RT) Danish 82c: T > 5cm : LR Failure 10%(RT) vs 34% (no RT) Deep fascia : LR Failure 6%(RT) vs 45% (no RT) Skin : LR Failure 8%(RT) vs 34% (no RT)
Recommendations -2 • PMRT not recommended in tumors less than 5 cm and negative axilla Risk of local recurrence is 9.2% without and 2.7% with PMRT (EBCTCG)
Recommendations -3 • Age, grade, LVI, hormone receptor status, number of nodes removed, extracapsular spread may affect LRC but indications unclear
Recommendations -4 • PMRT should encompass chest wall, supraclavicular, infraclavicular area and axillary apex • After complete dissection of the axilla (level I and II) avoid radiating the axilla • Definite recommendations to include IMC (Investigational in an EORTC trial) • Use modern techniques, avoid heart and lungs • Acute effects: skin reactions. Late effects-cardiac(relative hazard 3.2 times) /pulmonary (3%) /rib fractures/brachial plexopathy are rare
ISODOSE DISTRIBUTION Prescription Isodose (100%) 1cm off axis
Recommendations -5 • Sequencing of PMRT and systemic therapy unclear. Do not administer concomitantly with anthracyclines or taxanes
Delay in RT (for giving CT before RT) reduces Local controlMeta-Analysis of 1927 breast cancer patients (mostly BCT)
Univ. Med Centre, Utrecht, The Netherlands, Fiets et al 154 patients (BCT – 107, MRM - 47) ref during 1996-99 RT 50Gy / 25# (BCT: 16Gy boost); Nodal RT in 71 patients Chemo if indicated; CMF or AC on Med Oncologist’s discretion RT alone (n=61) RT + CMF (n=51) RT + AC (n=42) Prospective detailed evaluation of acute Toxicities Before, During & After RT (up to 6 months)
RT alone (n=61) RT + AC (n=42 RT + CMF (n=51) Incidence of SEVERE (Grade 2- 4)Acute Toxicities Moist Desquamation 21% 41% 70% Dysphagia 5% 18% 36% Dyspnoea 17% 43% 43% R. Pneumonitis 2% 4% 5% (NS) Malaise 40% 61% 62% Anorexia 2% 20% 41% Fever 0% 10% 11%