Download

1 / 23
230 likes | 360 Views
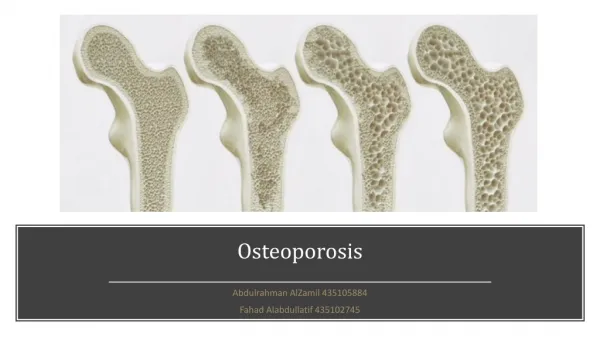
Osteoporosis. Low bone mass and structural deterioration of bone tissue leading to increase susceptibility to fracture. 9 million fragility fractures annually worldwide 300,000/yr in the UK.

E N D
Low bone mass and structural deterioration of bone tissue leading to increase susceptibility to fracture. • 9 million fragility fractures annually worldwide • 300,000/yr in the UK
Direct medical costs from fragility fractures in UK was estimated at £1.8 billion in 2000, potential to increase to £2.2 billion in 2025. • Hip fracture nearly always requires hospitalisation, is fatal in 20% of cases and permanently disables 50%
Fragility fracture • Result from mechanical forces that would not normally result in fracture – low level trauma • WHO define this as fall from standing height or less • Most commonly occur in spine, hip and wrist. • Can also occur in arm, pelvis ribs and other bones
Targeting osteoporosis • Primary prevention in at risk group • Secondary prevention following fragility fracture if appropriate. • QOF • Nice guidance from Aug 2012 suggests we should risk assess all those with risk factors
Secondary prevention = easy • If fragility fracture. • Bisphosphonates if > 75 • DEXA if < 75. treat if T score < 2.5
QOF • OST1: The practice can produce a register of patients: • Aged 50–74 years with a record of a fragility fracture after 1 April 2012 and a diagnosis of osteoporosis confirmed on DXA scan, and • Aged 75 years and over with a record of a fragility fracture after 1 April 2012. • OST2: The percentage of patients aged between 50 and 74 with a fragility fracture in whom osteoporosis has been confirmed on a DXA scan and who are currently being treated with an appropriate bone-sparing agent. • OST3: The percentage of patients aged 75 years and over with a fragility fracture and who are currently treated with an appropriate bone-sparing agent.
Primary prevention – targeted risk assessment (NICE 146) • All woman>65, Men>75 • All over > 50 in presence of RF’s • Do not routinely assess fracture risk in people <50 unless major RF’s (frequent use oral steroids, untreated premature menopause or fragility fracture)
Risk factors • Previous fragility fracture • Steroids • History of falls • Family hx of hip fracture • Low BMI (<18.5) • Smoking • Alcohol intake >14U/week for women, >21U/week for men • Other causes of secondary osteoporosis (i.e. hyperparathyroid, cushings, hypogonadism, hyperthyroid, rheumatoid, inflammatory bowel etc)
FRAX www.shef.ac.uk/FRAX/tool.jsp take you to national osteoporosis guideline group (NOGG) website tells you what to do. • NICE say all at high risk need DEXA though NOGG suggests some just treat. • QFracture www.qfracture.org (no NOGG link so harder to interpret) • Consider osteoporosis
Steroids > 3 months or 3-4 short courses/year > 15mg • Give bisphosphonates + D3/Ca in all aged > 65 • Everyone else needs DEXA + steroids if T score < -1.5
Interpreting DEXA • T score < -2.5 = osteoporosis need Rx • T score • -1 - -1.5 = mild osteopenia (rescan 15 yrs) -1.5 – 2 = moderate osteopenia (10 yrs) - 2 - -2.5 = severe osteopenia (1 yr)
Treatment • TFT, FBC, ESR, CRP, LFT at diagnosis • ? Enough calcium / vit D (should they have bone profile/ vit D levels) • In reality give all Vit D/ calcium replacement • Alendronate = 1st line (£13.20/yr) • NICE has complex decision making if intolerant to this based on cost - ? Ignore • Consider etidronate, risedronate (approx £300) • If still intolerant I would refer ? Strontium ranelate, zoledronate, raloxifene
Lifestyle advice – stop smoking. Weight bearing exercise. • At present fire and forget • No need for repeat DEXA • ? How long for? Probably 5-10 years then monitor with DEXA but controvertial + no clear guidelines
How to give? • Empty stomach with large glass of water • Remain upright and do not eat for 30 minutes after taking. • Slight increased risk of oesophageal Ca (NNH 1000) reduced by taking correctly
What about vitamin D • DOH recommends supplements if • 0-6 months breast fed deficient mum (280IU / 7 micrograms) • 7 months to 5 years – all (dose as above) • > 65 years old, pregnant, lactating, poor sun exposure!!!! (400IU, 10 micrograms)
Healthy start for children and eligible pregnant adults • Abidec – kids • Pregnacare – pregnancy • Elderly – otc vit D or Pro D3
When to test? • Symptoms not screening. • Aches and pains. • Hypocalcaemia. • Unexplained raised PTH (secondary hyperparathyroidism) • High risk populations offer advice / OTC supplements (but not cost effective to screen).
Lifestyle advice • Sun exposure • Oily fish, red meat, egg yolk • Fortified margarine, breakfast cereals
When to test? • Symptomatic • Check bloods for Ca, Phosphate, LFT, U+E, 25-OH vit D • 25-50 nmol/L = insufficient. CONTROVERTIAL - Offer lifestyle advice and supplements OTC. Though if lower range and severe symptoms consider high dose treatment • < 25 nmol/L = deficient.
If deficient (< 25nmol/L) • Refer if: • CKD stage 4-5 • Malabsorption • Atypical biochemistry (i,e hypercalcaemia could have primary hyperparathyroidism) • Skeletal deformity/ short stature • Focal bone pain • Unexplained severe deficiency • Failure to respond after 3 months treatment
Treatment • Pro D3 20000 units daily for 15-30 days • Or 100000 units weekly for 3-6 weeks (compliance) • After this low dose maintenance rx – fultium D3 – 800 – 1600 units daily • (OTC preparations if not tolerated) • Check Ca, phosphate and ALP at 2 months • Don’t check Vit D routinely if symptoms resolve
Osteoporosis – this about risk assessment and DEXA • Use FRAX and NOGG • Vit D supplements recommended in various age groups • Vit D treatment is controvertial but only check if symptomatic and only treat aggressively if deficient