Download
1 / 166
1.68k likes | 1.97k Views
Pituitary Function and Pathology. Dr Duncan Fowler The Ipswich Hospital. Overview. Anatomy Physiology Assessment of pituitary function: static and dynamic tests Clinical scenario’s: Cushing’s Disease Acromegaly Prolactinoma Apoplexy. Learning Objectives.

E N D
Pituitary Function and Pathology Dr Duncan Fowler The Ipswich Hospital
Overview • Anatomy • Physiology • Assessment of pituitary function: static and dynamic tests • Clinical scenario’s: • Cushing’s Disease • Acromegaly • Prolactinoma • Apoplexy
Learning Objectives • Describe pituitary anatomy and endocrine physiology • Describe methods for assessing pituitary function using static and dynamic testing • Describe the new standard for the measurement of growth hormone & its effects on clinical criteria • Be are of the importance of screening for macroprolactin
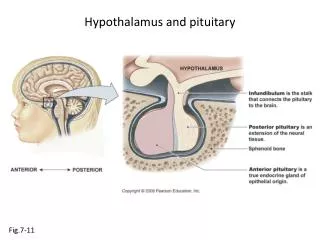
Hypothalamo-pituitary anatomy • Hypothalamus is the part of the diencephalon associated with visceral, autonomic, endocrine affective and emotional behaviour • Ventral portion forms the infundibulum • Posterior to this is the median eminence – the final point of convergence of pathways from the CNS on the endocrine system and is vascularised by the primary capillaries of the hypothalamo-hypophyseal portal vessels
Terminology • Adenohypophysis = anterior pituitary controlled by releasing and inhibiting factors released from nerves in the median eminence into the hypophyseal portal vessels which carry them to the pituitary • Neurohypophysis = posterior pituitary. It is an extension of the CNS. Its function is controlled by direct neural connection to the hypothalamus
Presentation • Hormonal hypersecretion e.g. Acromegaly • Hormonal deficiency e.g amenorrhoea • Local pressure effects: headaches, visual field loss – bitemporal hemianopia – bump into things
Identical chain but specific chain – non covalently associated • Luteinising hormone (LH) • Follicular stimulating hormone (FSH) • Thyroid stimulating hormone (TSH) • (human chorionic gonadotrophin – hCG) Potential for cross reaction e.g. hyperemesis
Stimulators of TSH • Pulsatile release (~9 x/24 hours) – amplitude at night • Secretion stimulated by thyrotrophin releasing hormone (TRH) released into the hypohyseal portal vessels in the median eminence • (TRH also stimulates prolactin release and in some circumstances growth hormone)
Inhibitors of TSH • Thyroid hormones directly inhibit TSH (and to a lesser extent TRH) release • This can prevent the action of TRH which is basis for TRH test • Dopamine and somatostatin inhibit release ?physiologically important but useful clinically for TSHomas
Stimulators of LH/FSH • Pulsatile secretion • Stimulated by pulsatile secretion of gonadotrophin secreting hormone (GnRH) into the hypophyseal portal vessels • GnRH release is complex and very susceptible to stress and changes to nutrition and energy homeostasis e.g. hypothalamic hypogonadotrophic hypogonadism seen in weight loss or extreme exercise
Inhibitors of LH/FSH • Oestradiol and progesterone inhibit LH release directly and via GnRH but in the follicular phase oestradiol becomes stimulatory inducing a surge of LH and ovulation (positive feedback) • Inhibin from the ovary inhibits FSH release • In the late follicular phase inhibin and oestradiol inhibit FSH release • In men equally complex but more static
Stimulators of ACTH • ACTH is a single chain peptide cleaved from POMC along with MSH and endorphin (hence pigmentation in Addison’s) • Secreted in pulsatile fashion in response to corticotrophin releasing hormone (CRH) – determines set point around which cortisol feedback works • Circadian rhythm with superimposed effects of stress
Inhibitors of ACTH • Feedback from cortisol mainly directly on pituitary but also on CRH release • Other adrenal androgens whose secretions are enhanced by ACTH do not have a feedback effect e.g. in congenital adrenal hyperplasia • Feedback can be imitated by synthetic glucocorticoids e.g. Dexamethasone (used in suppression testing – tumorous corticotrophs less susceptible to feedback)
Stimulators of GH release • Growth hormone releasing hormone (GHRH) stimulates synthesis/release of GH in pulsatile fashion – mostly at night • Ghrelin may have a role in secretion • GH exerts its effects directly and via IGF-1 production by the liver • Hypoglycaemia stimulates GH release (basis of ITT for GH deficiency) • Amino acids stimulate GH release (arginine can be used if ITT contraindicated)
Inhibitors of GH release • Somatostatin inhibits GH release • Feedback from GH and IGF-1 inhibit GH release at pituitary and hypothalamic level • Free fatty acids inhibit GH release • Glucose inhibits GHRH and GH release (basis of GH suppression test for acromegaly)
Stimulators of prolactin release • Released in pulsatile fashion especially at night • No direct stimulatory factor • Prolactin release is under tonic inhibitory control • Oestrogens cause hyperplasia of lactotrophs (hence care with COC with prolactinomas) & enhance prolactin release • TRH causes release of prolactin as well as TSH but this is not physiological
Inhibitors of prolactin release • Dopamine tonically inhibits release • Impeding the hypophyseal portal circulation causes enhanced prolactin release in contrast to other pituitary hormones. Prolactin can rise to 2000 mU/l due to this ‘stalk effect’ • Dopamine antagonist drugs e.g. metoclopramide, tricyclic antidepressants can stimulate prolactin release
Prolactin • TFT’s • LH/FSH and testosterone/oestradiol – but timing important • IGF-1 (for GH) • Cortisol – random samples not usually helpful –usually done 9am • Serum and urine osmolality (plus additional tests to investigate SIADH)
Prolactin • If in doubt measure basal prolactin on 3 occasions
Macroprolactin • Non-bioactive prolactin: monomer of prolactin and IgG molecule with prolonged clearance rate • Accounts for 10-30% of hyperprolactinaemia • Some but not all assay systems claim to detect macroprolactin but there are doubts • Treat sera with polyethylene glycol to precipitate out immunoglobulins then re assay for prolactin • Screening recommended for all hyperprolactinaemic sera (Clin Endo 71,466)
Clinical relevance • Macroprolactin is not biologically active – people with it have normal gonadal function • If someone with gonadal dysfunction due to another cause is found to have “hyperprolactinaemia” due to macroprolactin: • inappropriate dopamine agonist treatment • imaging of the pituitary undertaken revealing incidentalomas (found in up to 10%) and unnecessary investigation and treatment
Prevalence of macroprolactinaemiaClin Endo 71;702 (2009) • 1330 hospital workers in Japan screened for hepatitis B • 49 of 1330 (3.7%) had macroprolactin • 15 (30.6%) of these 49 had hyperprolactinaemia – all had normal monomeric prolactin on PEG precipitation • 29 of 1281 (2.26%) without macroprolactin had (true) hyperprolactinaemia
Of the 44 hyperprolactinaemias, 15 had macroprolactinaemia (34%) • Nobody had macroprolactinaemia and raised free prolactin • All sera with macroprolactin showed complexes of prolactin and IgG – most had anti PRL Abs, with others showing a variety of prolactin complexes
Total PRL-free PRL/total PRL x 100 : if >57% = macroprolactinaemia
IgG bound 100% Anti PRL Abs 76% Glycosylated PRL 20% (?relevant)
Of the 12 sera without antiPRL Abs Covalent disulfide bonds may be involved Suggests non covalent binding of IgG to prolactin and/or other proteins or aggregation of PRL
TFT’s - Lack of elevation of TSH in the presence of low T4 • Indicates pituitary or hypothalamic cause of hypothyroidism – or sick euthyroid syndrome • Same pattern can occur in 1st few months of treatment of thyrotoxicosis: T4 and T3 can be reduced below normal by carbimazole yet TSH remains suppressed
Sick euthyroid syndrome • Any severe non thyroidal illness can cause • fT4 low • fT3 is low or undetectable – reduced more than T4 • TSH is usually normal but may be low • Reverse T3 is normal or elevated • Preferential production of rT3, reduced binding globulins and circulating thyroid homone binding inhibitors • Clinical judgement but more common than 2º hypothyroidism
TFT’s - Elevated fT4 and fT3 with failure of suppression of TSH Discordant T4 and T3 • Interfering antibodies – no clinical signs • Amiodarone • Familial dysalbuminaemic hyperthyroxinaemia
TFT’s - Elevated fT4 and fT3 with failure of suppression of TSH Other • Intermittent T4 therapy • Resistance to thyroid hormone* • TSH secreting tumour* • Acute psychiatric illness
Gonadotophins • In menstruating females tests not usually needed • Day 21 progesterone gives information on ovulation • High prolactin can suppress gonadotrophin secretion • In males if 9am testosterone is normal then gonadotrophin secretion is adequate
Growth hormone • Random tests not helpful due to pulsatile secretion • Need dynamic testing or IGF-1
GH assays • Evolved from polyclonal RIA’s to 2 site monoclonal antibody non-isotopic assays with enhanced sensitivity • Accurately quantify previously undetectable values • Do we need age and gender dependent reference ranges ?
Growth Hormone Units – a mess! • Previous standard not pure & contained a number of isoforms: 22kD, 20kD and dimers/oligomers • UKNEQAS showed between method variation increasing from 1994 to 1998 from 17 to 30% - most negatively biased assay reported values ½ that of most positively biased • In past: UK used mU/l and US mcg/l • Various conversion factors between 2 and 3 used • No simple conversion factor suitable
New standard • EU legislation means all lab results must be traceable to a defined material (98/79/EC) • Since 2001 new international standard in use (IS98/574): 22kD GH of >95% purity • Now we should use mcg/l of IS98/574 • We should not use mIU/l but assigned conversion factor is 3.0 IU/mg • Criteria need to be looked at again
9am cortisol • ‘normal’ cortisol concentration does not exclude dysfunction • >500 nmol/l makes deficiency unlikely (unless v sick) • <100 nmol/l likely to be abnormal. Coincident ACTH can help • Need further testing • Salivary cortisol may become more important
Posterior Pituitary • Paired serum and urine osmolality on rising • Normal serum osmolality 280-295 mosmol/kg and concentrated urine (ratio >2:1) excludes DI • In DI serum osmolality is raised and urine ratio is <2.0 (but still may be more than serum in mild cases) • Most need water deprivation test