Download
1 / 32
400 likes | 1.15k Views
Whiplash Injuries Evaluation and treatment. Vikram B. Patel, MD FIPP DABIPP Medical Director] ACMI Pain Care Algonquin, Illinois. Disclaimer. No financial relationships with any manufacturing companies or pharmaceutical companies Some indications may not be FDA approved

E N D
Whiplash InjuriesEvaluation and treatment Vikram B. Patel, MD FIPP DABIPP Medical Director] ACMI Pain Care Algonquin, Illinois
Disclaimer • No financial relationships with any manufacturing companies or pharmaceutical companies • Some indications may not be FDA approved • Mention of any trade names is purely for the sake of clarification and simplicity • Personal disclaimer (!)
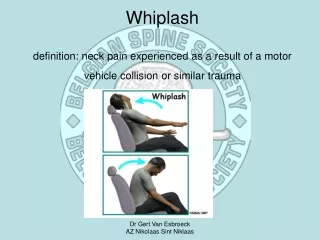
Whiplash Injuries • Injury due to trauma to the cervical spine • The term "whiplash" was first used in 1928. • Mechanism of injury • Flexion • Extension • Vertical compression • Direct trauma • Mixed mechanisms • Trivial to fatal severity
Cervical Spine Anatomy Atlanto-Axial Joint
Cervical Spine Injuries • Trauma • 10-15% of E.R. visits • Most injuries at C6 C 7 level (~50%) • 1/3rd injuries at C2 level • Hanging • Hangman’s fracture (C2) • Direct trauma • Verticle fall (Jefferson fracture – C1) • Object hitting from top or horizontally
Flexion Injuries • Head-on collision • Falling face forward • Forcible forward flexion • Structures primarily injured • Disc • Nerve root • Vertebral body • Compression • Subluxation
Extension injury • Rear ended collision • Falling backwards • Forcible extension of the neck • Structures injured • Facet joints • Muscles • Vertebral artery
Mixed Injuries • Flexion-rotation • Extension-rotation • Vertical compression • Structures injured • Multiple structures • Muscles and ligaments
Clinical Presentation • Neck pain • Upper back pain • Headaches • Radiating pain to the occiput, shoulders, arms • Neurological symptoms • Numbness, weakness • Remote signs and symptoms • Leg weakness and numbness • Bowel or bladder symptoms
Evaluation • History • Mechanism of injury (Flexion, extension or mixed) • Aggravating and relieving factors • Additional symptoms and complains • Bowel or bladder symptoms
Evaluation • Physical examination • Muscolo-skeletal exam • Range of motion (cervical spine and shoulders + arms) • Palpation • Neurological exam • Sensory and motor examination • Reflexes • Gait • Always assume spinal cord trauma unless proven otherwise
Management • Based on injured structures • Immobilization • Investigations • Plain x-ray • MRI • MRA • EMG/NCV • Multi-modal approach • Interventions • Physical therapy • Pharmaceuticals
Flexion injuries • Disc injury • Surgical approach • Percutaneous decompression • Nerve root • Steroid injections • Cervical epidural • Transforaminal approach vs. interlaminar approach
Extension Injuries • Subluxations • Surgical approach • Facet joint injury • Direct joint injection • Neuro-ablative techniques • Muscular injury • Physical therapy (with or without TPI) • Pharmaceuticals
Cervical Facet Syndrome • Symptoms Neck pain Headache Shoulder pain Suprascapular pain Scapular pain Upper arm pain • Signs Decreased range of motion of then neck Pain on neck extension, rotation Decreased discomfort with forward flexion Tenderness over the affected joint (lateral palpation)
Distribution of Symptoms • C2-C3: occiput and cervical spine • C3-C4: Neck • C4-C5: Lateral aspect of the name and shoulder • C5-C6: Arm • C6-C7: Shoulder, and into back, as far down as scapula
Cervical Facet Syndrome Raj et al. Practical Management of Pain
Summary • Whipash injuries are very common in MVAs • Very high mortality rate with upper cervical spine injuries • High morbidity with lower cervical spine injuries • MRI is the best modality for evaluation • Surgical interventions should be considered earlier due to risk of spiral cord trauma • Neurological assessment is a must (upper and lower extremities) • Effective management includes multimodal approach
Thank You • Questions??