Download
1 / 1
10 likes | 104 Views
No. 120. The Role of Insulin in Castrate Resistant Progression of Advanced Prostate Cancer in Patients Receiving Long-Term Androgen Deprivation Therapy. Dr Ian McKenzie 1,2 , Prof Colleen Nelson 1 , Dr Peter Swindle 2

E N D
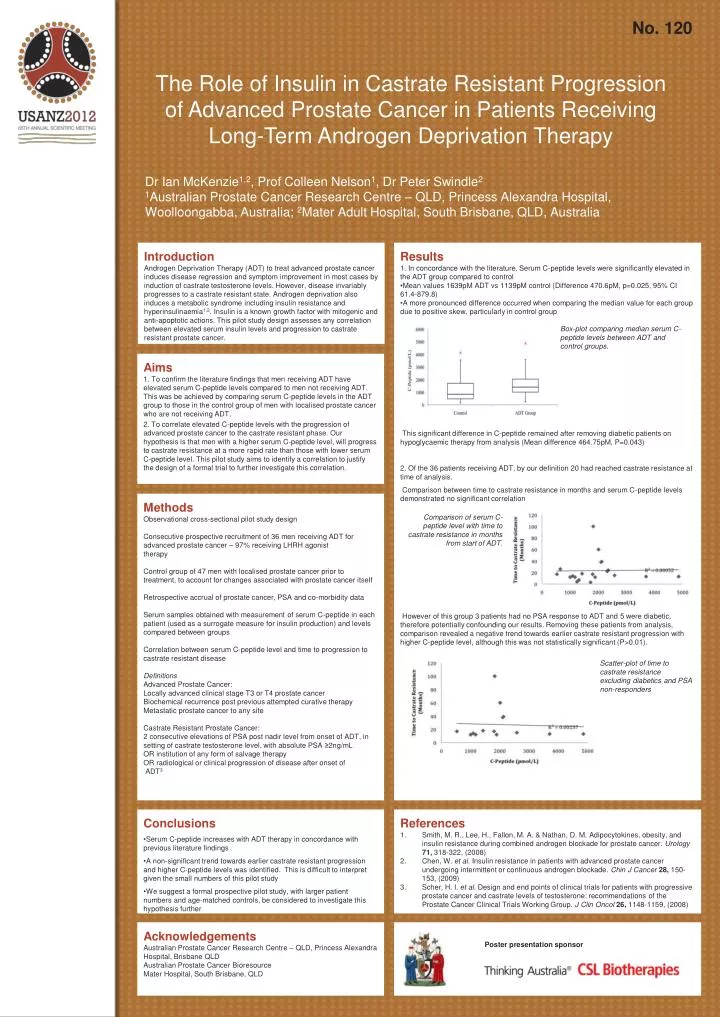
No. 120 The Role of Insulin in Castrate Resistant Progression of Advanced Prostate Cancer in Patients Receiving Long-Term Androgen Deprivation Therapy Dr Ian McKenzie1,2, Prof Colleen Nelson1, Dr Peter Swindle2 1Australian Prostate Cancer Research Centre – QLD, Princess Alexandra Hospital, Woolloongabba, Australia; 2Mater Adult Hospital, South Brisbane, QLD, Australia Introduction Androgen Deprivation Therapy (ADT) to treat advanced prostate cancer induces disease regression and symptom improvement in most cases by induction of castrate testosterone levels. However, disease invariably progresses to a castrate resistant state. Androgen deprivation also induces a metabolic syndrome including insulin resistance and hyperinsulinaemia1,2. Insulin is a known growth factor with mitogenic and anti-apoptotic actions. This pilot study design assesses any correlation between elevated serum insulin levels and progression to castrate resistant prostate cancer. • Results • 1. In concordance with the literature, Serum C-peptide levels were significantly elevated in the ADT group compared to control • Mean values 1639pM ADT vs 1139pM control (Difference 470.6pM, p=0.025, 95% CI 61.4-879.8) • A more pronounced difference occurred when comparing the median value for each group due to positive skew, particularly in control group • This significant difference in C-peptide remained after removing diabetic patients on hypoglycaemic therapy from analysis (Mean difference 464.75pM, P=0.043) • 2. Of the 36 patients receiving ADT, by our definition 20 had reached castrate resistance at time of analysis. • Comparison between time to castrate resistance in months and serum C-peptide levels demonstrated no significant correlation • However of this group 3 patients had no PSA response to ADT and 5 were diabetic, therefore potentially confounding our results. Removing these patients from analysis, comparison revealed a negative trend towards earlier castrate resistant progression with higher C-peptide level, although this was not statistically significant (P>0.01). Box-plot comparing median serum C-peptide levels between ADT and control groups. Aims 1. To confirm the literature findings that men receiving ADT have elevated serum C-peptide levels compared to men not receiving ADT. This was be achieved by comparing serum C-peptide levels in the ADT group to those in the control group of men with localised prostate cancer who are not receiving ADT. 2. To correlate elevated C-peptide levels with the progression of advanced prostate cancer to the castrate resistant phase. Our hypothesis is that men with a higher serum C-peptide level, will progress to castrate resistance at a more rapid rate than those with lower serum C-peptide level. This pilot study aims to identify a correlation to justify the design of a formal trial to further investigate this correlation. Methods Observational cross-sectional pilot study design Consecutive prospective recruitment of 36 men receiving ADT for advanced prostate cancer – 97% receiving LHRH agonist therapy Control group of 47 men with localised prostate cancer prior to treatment, to account for changes associated with prostate cancer itself Retrospective accrual of prostate cancer, PSA and co-morbidity data Serum samples obtained with measurement of serum C-peptide in each patient (used as a surrogate measure for insulin production) and levels compared between groups Correlation between serum C-peptide level and time to progression to castrate resistant disease Definitions Advanced Prostate Cancer: Locally advanced clinical stage T3 or T4 prostate cancer Biochemical recurrence post previous attempted curative therapy Metastatic prostate cancer to any site Castrate Resistant Prostate Cancer: 2 consecutive elevations of PSA post nadir level from onset of ADT, in setting of castrate testosterone level, with absolute PSA ≥2ng/mL OR institution of any form of salvage therapy OR radiological or clinical progression of disease after onset of ADT3 Comparison of serum C-peptide level with time to castrate resistance in months from start of ADT. Scatter-plot of time to castrate resistance excluding diabetics and PSA non-responders • Conclusions • Serum C-peptide increases with ADT therapy in concordance with previous literature findings • A non-significant trend towards earlier castrate resistant progression and higher C-peptide levels was identified. This is difficult to interpret given the small numbers of this pilot study • We suggest a formal prospective pilot study, with larger patient numbers and age-matched controls, be considered to investigate this hypothesis further References Smith, M. R., Lee, H., Fallon, M. A. & Nathan, D. M. Adipocytokines, obesity, and insulin resistance during combined androgen blockade for prostate cancer. Urology 71, 318-322, (2008) Chen, W. et al. Insulin resistance in patients with advanced prostate cancer undergoing intermittent or continuous androgen blockade. Chin J Cancer 28, 150-153, (2009) Scher, H. I. et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J ClinOncol26, 1148-1159, (2008) Acknowledgements Australian Prostate Cancer Research Centre – QLD, Princess Alexandra Hospital, Brisbane QLD Australian Prostate Cancer Bioresource Mater Hospital, South Brisbane, QLD Poster presentation sponsor






