Download
1 / 40
420 likes | 653 Views
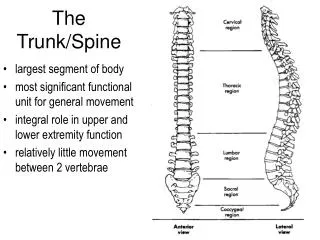
Managing the Geriatric Spine. Orthotic Management of the Geriatric Spine. Andrew J Mills MBAPO MISPO Orthotist. Managing the Geriatric Spine. Orthotic Management of Degenerative Scoliosis in Adults. Managing the Geriatric Spine. Prevalence of Scoliosis in Adults.

E N D
Managing the Geriatric Spine Orthotic Management of the Geriatric Spine Andrew J Mills MBAPO MISPO Orthotist
Managing the Geriatric Spine Orthotic Management of Degenerative Scoliosis in Adults
Managing the Geriatric Spine Prevalence of Scoliosis in Adults
Managing the Geriatric Spine Prevalence of Scoliosis in Adults • General Population • 0.3% – 0.5% in Children (of which 80% are idiopathic) • 2% – 4% above the age of 18 years • 9% in over 40 year olds • 30%+ in over 60 year olds • Patients with Low back Pain • Robin et al; Study 554 LBP Patients • 30% had scoliosis >10° in the 50 to 84 age group • And at 5 year follow up • - 40% had scoliosis >10° an additional 10% “
Managing the Geriatric Spine Types of Scoliosis in Adults Types of Scoliosis in Adults
Managing the Geriatric Spine Types of Scoliosis in Adults Two main types; 1. Adolescent Scoliosis in the Adult (ASA) 2. Degenerative De-Novo scoliosis (DDS) Important, however, to rule out scoliosis due to pathological disease prior to brace treatment
Managing the Geriatric Spine ASA 1 • Usually smaller flexible curves in younger adults 18-30 years old • Posture and Cosmetic issues are the main problem. • Pain can be an issue particularly in unbalanced curves. • Potential reducibility in both abnormal posture and Cobb.
Managing the Geriatric Spine ASA 2 • Usually larger more rigid curves in middle aged adults 30-40 • Pain and posture equally issues. • Pain can be an issue even in balanced curves. • Often start to see early degenerative changes • Intervention in ASA 2 could potentially to stop progression to ASA 3 • (This idea of early intervention is suggest by Schwab Spine 2002)
Managing the Geriatric Spine ASA 3 • Usually large, rigid curves in older adults 40+ • Pain is the primary issue. • Moderate to severe degenerative changes present. • Most commonly lumbar curves. • No previous history of scoliosis could indicate Degenerative De Novo Scoliosis DDS.
Managing the Geriatric Spine Degenerative De-Novo Scoliosis (DDS) • New curve in adult developed as a result of degenerative instability. • Usually lumbar curve, unbalanced. • Large, rigid curves in older adults 50+ • Pain is the primary issue. • Moderate to severe degenerative changes present.
Managing the Geriatric Spine Vertebral Rotation • Both ASA and DDS have vertebral rotation. • In ASA rotation of the vertebra is initially related to the 3D vertebral deformity
Managing the Geriatric Spine Rotary Subluxation • With DDS the vertebra are NOT deformed. • Instability allows one or more of them to rotate. • This rotation is greater than the normal coupling limits would allow. • Therefore it is considered a subluxation.
Managing the Geriatric Spine Rotary Subluxation • This subluxation is a typical feature of DDS. • It can appear latter on with ASA on top of the true rotational deformity.
Managing the Geriatric Spine • Research demonstrates that; • Cobb Magnitude and • Degenerative Changes • Menopause • Alone do not necessarily relate to Pain or Progression
Managing the Geriatric Spine Are there Biomechanical Factors relating to Pain and Progression that could be managed by Spinal Bracing?
Managing the Geriatric Spine Clinical & Radiological Features that relate to pain with Adult Scoliosis
Managing the Geriatric Spine Radiological features correlating with Pain • “Adult Scoliosis - A Quantitative Radiographic and Clinical Analysis”, Schwab et al. Spine 2002, • He identifies these correlations with pain: • Lateral vertebral olisthesis, (side slip) • L3 and L4 endplate obliquity angles, • Decrease in lumbar lordosis, • Increased thoraco-lumbar Kyphosis
Managing the Geriatric Spine Cobb angle correlation with pain • “Adult Scoliosis - A Quantitative Radiographic and Clinical Analysis”, Schwab et al. Spine 2002, • The Cobb angle of the scoliotic deformity had no statistically significant correlation to the VAS pain scores. • Suggests that; • Early intervention in a middle-aged adult with scoliosis may be preferable to treating advanced deformity in that same person once he or she has become elderly.
Managing the Geriatric Spine SagittalBalance “Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis” Glassman, et al. Spine 2003 • The most significant findings were: • Positive (anterior) Sagittal Balance • Greater pain • Diminished physical function • Poorer self image • - Poorer social function
Managing the Geriatric Spine Coronal Balance “Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis” Glassman, et al. Spine 2003 • The most significant findings were: • Coronal shift > 4 cm • - Poorer function • - Greater pain • Compared to patients with a coronal shift < 4 cm.
Managing the Geriatric Spine Glassman Study Non-correlation Findings “Correlation of Radiographic Parameters and Clinical Symptoms in Adult Scoliosis” Glassman, et al. Spine 2003 • No differences based on: • Curve magnitude • Apical rotation, • Or single vs. double major curves. • More favourable scores for thoracic curves versus thoracolumbar or lumbar curves
Managing the Geriatric Spine Severity Of Degeneration (DDD/Spinal Stenosis) • By its self severity of degeneration not a predictor of Pain or Progression • In combination with rotary subluxationit is a predictor for progression. • In combination with end plate obliquity it is a predictor for ongoing pain
Managing the Geriatric Spine Glassman/Schwab Studies Summary of Key Findings:
Managing the Geriatric Spine Glassman Schwab Studies Summary of Key Findings:
Managing the Geriatric Spine Orthotic Strategies Orthotic Strategies to manage pain and progression in Adult Scoliosis
Managing the Geriatric Spine Orthotic Strategies The primary bracing objectives in adult scoliosis do not relate to curve correction! • Primary objectives are to; • Improve/correct Sagittal imbalance. • Improve/correct Coronal imbalance. • Strengthen Spinal Muscles. • Reduce pathological mechanical loads. • Provide Dynamic Corrective Movement • Provide Postural Re-education • That ultimately reduce pain and progression!
Managing the Geriatric Spine Rigid Vs Dynamic Orthotic Treatment • Rigid • Muscle Atrophy causing further destabilization of the spine. • Limitation of movement • Self image issues • Comfort issues • Not well tolerated in long term use • Useful as a last resort in severe Neuro-degenerative cases • Dynamic • Muscle rehabilitation and stabilization • Allows movement • Not visible under clothing • Relatively comfortable • Suitable for long term use • Generally Not suitable for severe Neuro-degenerative cases
Managing the Geriatric Spine Dynamic Bracing Approach in Adults
Managing the Geriatric Spine Rigid Vs Dynamic Orthotic Treatment Clearly a dynamic bracing approach has significant advantages to a rigid one in Adults. • No issues with muscular atrophy • Possible to increase general muscle strength and core stability • Increases rather than limiting mobility • Allows sustainable improvement/corrections of coronal and sagittal imbalances key to reduction of pain an progression.
Managing the Geriatric Spine Dynamic Bracing Treatment Approach • To use case specific Corrective Movements for spinal rehabilitation and correction/improvement of to patient’s postural imbalances. • The Corrective Movement strategy is determined by the curve type, region of pain and plane of maximum postural imbalance. • The same basic brace components are utilized for all patients only the number, configuration and tensions of the corrective bands vary.
Managing the Geriatric Spine Corrective Movement Principle 2 3 1
Managing the Geriatric Spine Corrective Movement Principle 2 3 1
Managing the Geriatric Spine Postural Overcorrection Overcorrection of the Postural disorganisation Using Dynamic Forces Compressive forces Distractive forces
Managing the Geriatric Spine : Corrective Movement & Spinal Loading
Managing the Geriatric Spine SpineCor Treatment Classification, Corrective Movement & Brace in Place
Managing the Geriatric Spine SpineCor Treatment Brace Adjustment to Optimize Corrective Movement Clinically measureable objectives.
Managing the Geriatric Spine Indications for bracing • Degenerative De-Novo Scoliosis (DDS) • Adolescent Scoliosis in Adults (ASA) • Hyperkyphosis • Pain; particularly lower back pain associated with postural & spinal and deformities. i.e. hyperkyphosis, coronal/sagittal imbalance. • Postural Imbalance; correction/rehabilitation of abnormal postural alignment. • Progression; slow or prevent progression of spinal and postural deformities.
Managing the Geriatric SpinePatient Example A • 26 year old female, • Painful adolescent idiopathic scoliosis as an adult (ASA1). • Pain 7/10. • 32 deg right thoracic scoliosis. • 8 to 12 hours for 3 months • Gradual relief of pain to 2/10. • Improvement of 8 degrees to 24 deg. • Pain relief of 1-2/10 and spinal correction have been maintained for over 2 years . Courtesy of Dr Tom Pappas
Managing the Geriatric SpinePatient Example B • 47 year old female • Degenerative De-Novo Adult Scoliosis. (DDS) • Pain 7/10. • A 40 deg degenerative lumbar scoliosis. • Immediate relief of pain to 3/10. • Pain relief of 0-3/10 maintained for over 2 years • Note the improved left lateral shift showing “spinal off loading”. Courtesy of Dr Tom Pappas
Managing the Geriatric Spine The End Thank you