Download
1 / 34
340 likes | 461 Views
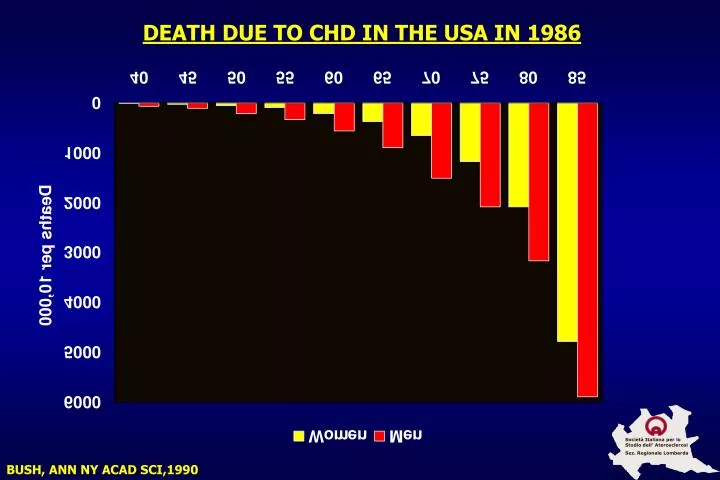
DEATH DUE TO CHD IN THE USA IN 1986. BUSH, ANN NY ACAD SCI,1990. PROCAM (MÜNSTER HEART STUDY): MENOPAUSE AND LIPID RISK FACTORS IN 45 TO 55 YEARS OLD WOMEN. Pre-Menopause Menopause P (n = 1537) (n = 2456) age (years) 48.3 ± 2.8 51.0 ± 3.0 < 0.001

E N D
DEATH DUE TO CHD IN THE USA IN 1986 BUSH, ANN NY ACAD SCI,1990
PROCAM (MÜNSTER HEART STUDY): MENOPAUSE AND LIPID RISK FACTORS IN 45 TO 55 YEARS OLD WOMEN Pre-Menopause Menopause P (n = 1537) (n = 2456) age (years) 48.3 ± 2.8 51.0 ± 3.0 < 0.001 BMI (kg/m2) 25.8 ± 4.3 26.4 ± 4.5 < 0.001 cholesterol (mg/dL) 221 ± 39 239 ± 41 < 0.001 triglycerides (mg/dL)* 88 99 < 0.001 LDL-C (mg/dL) 143 ± 36 158 ± 38 < 0.001 HDL-C (mg/dL) 59 ± 15 59 ± 16 n.s. chol./HDL-C ratio 4.02 ± 1.25 4.31 ± 1.32 < 0.001 *: geometric mean, n.s.: not significant
PROCAM (MÜNSTER HEART STUDY): MENOPAUSE AND HEMOSTATIC RISK FACTORS IN 45 TO 55 YEARS OLD WOMEN Pre-Menopause Menopause P (n = 229) (n = 307) fibrinogen (mg/dL) 265 ± 50 276 ± 56 < 0.001 D-dimer (mg/l)* 321 345 n.s. factor VIIc (mg/dL) 108 ± 26 120 ± 34 < 0.001 protein C (%) 111 ± 19 120 ± 24 < 0.001 plasminogen (%) 104 ± 14 106 ± 14 < 0.05 PAI-1 (U/l) * 2.22 2.48 < 0.05 vWF (%) 103 ± 35 96 ± 31 n.s. CRP (mg/dL)* 0.32 0.28 < 0.05 *: geometric mean
MAJOR RISK FACTORS FOR CHD AGE > 45 Y MALES AND > 55 Y FEMALES Family history of MI or sudden death: < 55 males < 65 females Cigarettes smoke Elevated blood pressure HDL-C < 35 mg/dL Diabetes mellitus HDL-C > 60 mg/dL NATIONAL CHOLESTEROL EDUCATION PROGRAM.CIRCULATION 1994;89:1329-445.
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda POSTMENOPAUSAL ESTROGEN/PROGESTIN INTERVENTIONS TRIAL (PEPI) • 875 HEALTHY POST-MENOPAUSAL WOMEN AGE 45-64 • PARALLEL INTERVENTION GROUPS: Placebo CEE 0.625 mg/d CEE 0.625 mg/d + MPA 10 mg/d x 12 d/mo CEE 0.625 mg/d + MPA 2.5 mg/d CEE 0.625 mg/d + MP 200 mg/d x 12 d/mo • ENDPOINTS: HDL-C Systolic blood pressure Fibrinogen Insulin JAMA 1995;273:199
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda PEPI TRIAL RESULTS • LIPOPROTEINS: • HDL-C increased in all active treatments (Greatest with CEE and CEE + MP) • LDL-C decreased equally in all treatment groups • Triglycerides increased equally in all treatment groups • SYSTOLIC BLOOD PRESSURE:increased similarly in all treatment groups • INSULIN:no difference in fasting or 2-hour insulin among all treatment groups • FIBRINOGEN:no difference among active treatment groups JAMA 1995;273:199
Baseline Baseline Run-in Run-in 3 months 3 months Oral Transdermal -5% 250 250 200 200 -15% +37% 150 150 mg/dL mg/dL 100 100 50 50 0 0 Total C LDL-C HDL-C TGL Total C LDL-C HDL-C TGL EFFECTS OF ORAL ESTROGENS ON SERUM LIPOPROTEINS IN POSMENOPAUSAL WOMEN BRANCHI A., 1998
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda PEPI Trial Results • LIPOPROTEINS: • HDL-C increased in all active treatments (Greatest with CEE and CEE + MP) • LDL-C decreased equally in all treatment groups • Triglycerides increased equally in all treatment groups • SYSTOLIC BLOOD PRESSURE:increased similarly in all treatment groups • INSULIN:No difference in fasting or 2-hour insulin among all treatment groups • FIBRINOGEN:No difference among active treatment groups JAMA 1995;273:199
ANTIATHEROGENE PROPERTILE OF ESTROGENS • Reduced proliferation of SMC and neo intima formation • Reduced production of collagen and elastin • Modulation of vasomotor response • Increased coronary responsed to vasodilatory stimuli • Increased prostacyclyn production by SMC • Reduction of plasma homocysteine levels
RELATIVE RISK AND 95% CI FROM STUDIES OF ESTROGEN USE TO PREVENT CHD Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda STAMPFER, NEJM, 1991
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda THE NURSES HEALTH STUDY: CHD RISK AND POSTMENOPAUSAL ESTROGEN + PROGESTIN USE • 59,337 women, age 30-55, followed for 16 years • Relative risk for CHD events in current estrogen users was 0.60, and current estrogen + progestin users was 0.39 • Length of HRT did not change risk reduction • Estrogen doses of 0.3 and 0.625 mg had the greatest benefit • Women 60-71 years old had as much benefit as younger women NEJM 1996;335:453
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda ESTROGEN REPLACEMENT IN POSTMENOPAUSAL WOMEN: NCEP RECOMMENDATIONS • Observational information suggests lower CHD risk in women on HRT • Experimental data suggests estrogen has beneficial effects on endothelial function • Oral estrogen can lower LDL-C and increase HDL-C • NCEP recommends that estrogen replacement can be used as alternative or adjunctive treatment to manage hypercholesterolemia in postmenopausal women.
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda HEART AND ESTROGEN/PROGESTIN REPLACEMENT STUDY (HERS) • Randomized, placebo-controlled trial of E/P therapy vs. placebo in 2,763 women with CHD; average age 67 years • Treatment was 0.625 mg CEE* + 2.5 mg medroxyprogesterone daily for 4 years • Primary endpoint: nonfatal MI and CHD death • Secondary endpoints: CABG, PTCA, unstable angina, CHF, PVD, TIA *CEE = conjugated equine estrogen; JAMA 1998;280:605-613
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda HEART AND ESTROGEN/PROGESTIN REPLACEMENT STUDY (HERS) CHANGES IN LIPID LEVELS AT 1 YEAR 15 10* 8* 10 5 2 0 Mean % change from baseline -2 -3 -5 Placebo Estrogen/progestin -10 -15 -14* -20 LDL-C HDL-C TG *P < 0.001 HULLEY S ET AL. JAMA 1998;280:605–613
Placebo (n=1383) Estrogen/Progestin (N=1380) CHD Death CHD Death + Nonfatal MI RH = 1.24 p = 0.23 RH = 0.99 p = 0.91 Incidence (%) Coronary Revascularisation or Unstable Angina Nonfatal MI RH = 0.88 p = 0.15 RH = 0.99 p = 0.46 THE HEART AND ESTROGEN/PROGESTIN REPLACEMENT STUDY (HERS) INCIDENCE OF CHD EVENTS IN TREATMENT AND PLACEBO GROUPS Follow-up (years) HULLEY ET AL. JAMA 1998; 280:605-613
15 10 Incidence (%) 5 Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda 0 5 (113) 3 (2,392) 4 (1,435) 0 (2,763) 1 (2,631) 2 (2,506) Follow-up, y (No. at risk) HEART AND ESTROGEN/PROGESTIN REPLACEMENT STUDY (HERS)CUMULATIVE INCIDENCE OF PRIMARY CHD EVENTS Estrogen/progestin Placebo Hulley S et al. JAMA 1998;280:605–613
SIDE-EFFECTS IN HERS STUDY Side-effects confirmed venous thrombosis deep vein thrombosis pulmonary embolus fatal pulmonary Embolus gallbladder disease oestrogen/ progestin (n=1380) 34 25 11 2 84 placebo (n=1383) 12 8 4 0 62 relative risk 2.3 3.1 2.8 - 1.4 P value 0.002 0.004 0.08 - 0.05 HULLEY ET AL. JAMA 1998; 280:605-613
Società Italiana per lo Studio dell’ Aterosclerosi Sez. Regionale Lombarda HERS RESULTS • No statistically significant difference between HRT • and placebo in both primary and secondary endpoints after 4 years. • Within first year, greater incidence in CHD events in HRT group. In years 3 and 4, lower CHD events in HRT group compared to placebo. • HRT lowered LDL 11% and increased HDL 10% compared to placebo. • Approximately 50% of randomized women were on lipid-lowering drugs. • Higher incidence of VTE and cholelithiasis in HRT group. JAMA 1998;280:605-613
CHD OUTCOMES DURING 6.8 YEARS OF HORMONE THERAPY (HERS II) • The higher risk of developing CHD in HERS was in the first two years of therapy. A decline occured between year 3 and 5. • HERS II was designed to verify whether the tendency to a reduction of CHD in HERS persisted in a longer follow up. • The HERS II study recruited 2.321 women (average 67 yearsof age) who gave their informed consent to continue therapy with the active drug or placebo. GRADY ET AL., JAMA 2002
CHD OUTCOMES DURING 6.8 YEARS OF HORMONE THERAPY (HERS II) JAMA, 2002
NON CHD OUTCOMES DURING 6.8 YEARS OF HORMONE THERAPY (HERS II) 1 JAMA, 2002
NON CHD OUTCOMES DURING 6.8 YEARS OF HORMONE THERAPY (HERS II) 2 JAMA, 2002
RISK AND BENEFITS OF ESTROGEN PLUS PROGESTIN IN HEALTHY POSTMENOPAUSAL WOMENPrincipal Results from the Women’s Health Initiative Randomized Controlled Trial • A randomized controlled primary prevention trial (planned duration 8.5 years) in which 16,608 postmenopausal women aged 50-79 years with an intact uterus at baseline were recruited by 40 US clinical centers in 1993-1998 • Participants received conjugated equine estrogens, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d or placebo JAMA, 2002
373,092 women initiated screening 18,845 provided consent and reported no isterectomy 16,608 randomized 8,506 assigned to Estrogen+Progestin 8,102 assigned to placebo • Status on April 30, 2002 • 7,608 alive • 276 unknown vital status • 218 deceased • Status on April 30, 2002 • 7,968 alive • 307 unknown vital status • 231 deceased PROFILE OF THE ESTROGEN+PROGESTIN COMPONENT OF THE WOMEN’S HEALTH INITIATIVE
WHI: CLINICAL OUTCOMES 1 JAMA, 2002
WHI: CLINICAL OUTCOMES 2 JAMA, 2002
WHI: CLINICAL OUTCOMES 3 JAMA, 2002
WHI: CAUSE OF DEATH JAMA, 2002
CONCLUSIONS • Overall health risk exceeded benefits from use of combined estrogen+progestin for an average 5.2 year follow-up among healthy postmenopausal women • Risk for CHD was largely limited to the 1° year of therapy, whereas risk for Stroke and Venous Thromboembolism continued throughout the 5 years of therapy and may reflect prothrombotic and proinflammatory effects of progestins • Risk for breast cancer was associated with the duration of treatment • The risk-benefit profile of combined HRT is not consistent with the requirements for primary prevention of chronic diseases
MENOPAUSAL HORMONE REPLACEMENT THERAPYAND RISK OF OVARIAN CANCER Study Design: cohort study on 44.241 post menopausas women Aim: to address whether the estrogen + progestin treatment could modify the risk of developping ovary cancer LACEY, JAMA 2002
HORMONAL REPLACEMENT THERAPY AND OVARIAN CANCER LACEY, JAMA 2002
INTERVENTION STUDIES AIMED AT THE PREVENTION OF CORONARY HEART DISEASE (SUBGROUPS OF WOMEN) 4S: The Lancet 1994;344:1383-1389 Care: Sacks FM et al. N Engl J Med 1996;335:1001-1009 AFCAPS/TexCAPS: Downs JR et al. JAMA 1998;279:1615-1622
Relative Risk IC 95% GROUPS SIMVA PLACEBO (10269) (10267) SIMVA better Placebo better AGE (YEAR) < 65 838 1093 65 - 69 516 677 2 Het = 4.4 3 70-74 550 628 >75 138 208 GENDER Male 1676 2148 2 Het = 0.4 1 Female 366 458 All patients 2042 2606 24% SE 2.6 (19.9%) (25.4%) (2P<0.00001) 0.4 0.6 0.8 1.0 1.2 1.4 SIMVASTATIN: SECONDARY ENDPOINT VASCULAR EVENTS BY AGE AND GENDER STATIN worse
HORMONAL REPLACEMENT THERAPY (WHEN TO BE USED) • Menopausal symptoms (vasomotor, urogenital or vaginal atrophy, mood disturbance) • High risk of osteoporosis • Early menopause