Download
1 / 1
10 likes | 105 Views
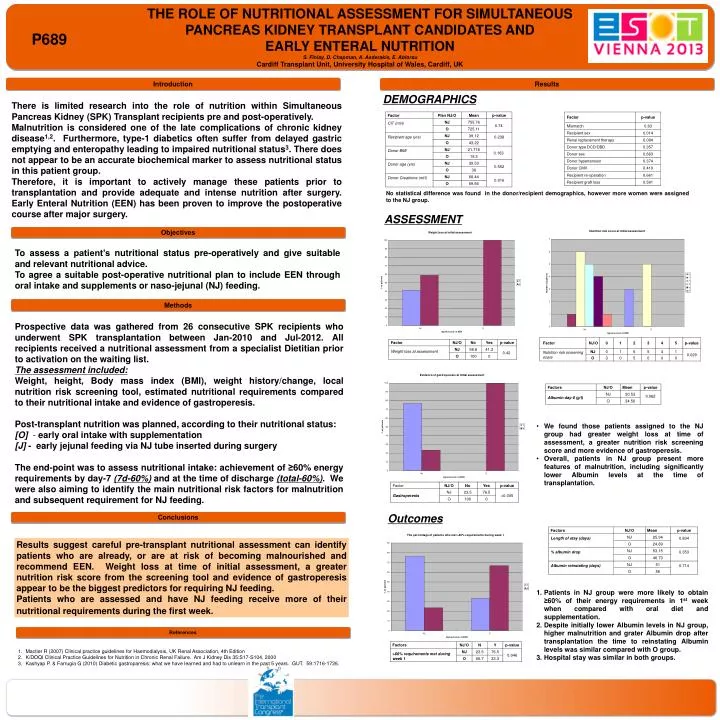
THE ROLE OF NUTRITIONAL ASSESSMENT FOR SIMULTANEOUS PANCREAS KIDNEY TRANSPLANT CANDIDATES AND EARLY ENTERAL NUTRITION S. Finlay, D. Chapman, A. Asderakis, E. Ablorsu Cardiff Transplant Unit, University Hospital of Wales, Cardiff, UK. P689. Replace with logo. Introduction. Results.

E N D
THE ROLE OF NUTRITIONAL ASSESSMENT FOR SIMULTANEOUS PANCREAS KIDNEY TRANSPLANT CANDIDATES AND EARLY ENTERAL NUTRITION S. Finlay, D. Chapman, A. Asderakis,E. Ablorsu Cardiff Transplant Unit, University Hospital of Wales, Cardiff, UK P689 Replace with logo Introduction Results DEMOGRAPHICS There is limited research into the role of nutrition within Simultaneous Pancreas Kidney (SPK) Transplant recipients pre and post-operatively. Malnutrition is considered one of the late complications of chronic kidney disease1,2. Furthermore, type-1 diabetics often suffer from delayed gastric emptying and enteropathy leading to impaired nutritional status3. There does not appear to be an accurate biochemical marker to assess nutritional status in this patient group. Therefore, it is important to actively manage these patients prior to transplantation and provide adequate and intense nutrition after surgery. Early Enteral Nutrition (EEN) has been proven to improve the postoperative course after major surgery. No statistical difference was found in the donor/recipient demographics, however more women were assigned to the NJ group. ASSESSMENT Objectives To assess a patient’s nutritional status pre-operatively and give suitable and relevant nutritional advice. To agree a suitable post-operative nutritional plan to include EEN through oral intake and supplements or naso-jejunal (NJ) feeding. Methods Prospective data was gathered from 26 consecutive SPK recipients who underwent SPK transplantation between Jan-2010 and Jul-2012. All recipients received a nutritional assessment from a specialist Dietitian prior to activation on the waiting list. The assessment included: Weight, height, Body mass index (BMI), weight history/change, local nutrition risk screening tool, estimated nutritional requirements compared to their nutritional intake and evidence of gastroperesis. Post-transplant nutrition was planned, according to their nutritional status: [O] - early oral intake with supplementation [J] - early jejunal feeding via NJ tube inserted during surgery The end-point was to assess nutritional intake: achievement of ≥60% energy requirements by day-7 (7d-60%) and at the time of discharge (total-60%). We were also aiming to identify the main nutritional risk factors for malnutrition and subsequent requirement for NJ feeding. • We found those patients assigned to the NJ group had greater weight loss at time of assessment, a greater nutrition risk screening score and more evidence of gastroperesis. • Overall, patients in NJ group present more features of malnutrition, including significantly lower Albumin levels at the time of transplantation. Outcomes Conclusions Results suggest careful pre-transplant nutritional assessment can identify patients who are already, or are at risk of becoming malnourished and recommend EEN. Weight loss at time of initial assessment, a greater nutrition risk score from the screening tool and evidence of gastroperesis appear to be the biggest predictors for requiring NJ feeding. Patients who are assessed and have NJ feeding receive more of their nutritional requirements during the first week. • Patients in NJ groupwere more likely to obtain ≥60% of their energy requirements in 1st week when compared with oral diet and supplementation. • Despite initially lower Albumin levels in NJ group, higher malnutrition and grater Albumin drop after transplantation the time to reinstating Albumin levels was similar compared with O group. • Hospital stay was similar in both groups. References • Mactier R (2007) Clinical practice guidelines for Haemodialysis, UK Renal Association, 4th Edition • K/DOQI Clinical Practice Guidelines for Nutrition in Chronic Renal Failure. Am J Kidney Dis 35:S17-S104, 2000 • Kashyap P. & Farrugia G (2010) Diabetic gastroparesis: what we have learned and had to unlearn in the past 5 years. GUT. 59:1716-1726.