Download
1 / 30
0 likes | 58 Views
Novel treatment of heart failure in diabetic patients

E N D
Treatment of HF in diabetic patients Professor / Mohammed Ahmed Bamashmos Professor of Internal Medicine and Endocrinology Faculty of Medicine ( Sanaa University
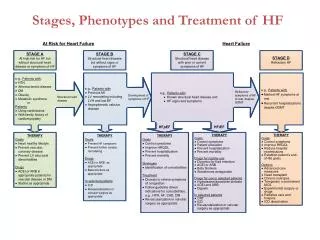
prevalence and risk factors the prevalence of HF in patients with DM is between 9% and 22%, which is 4 times higher than the general population, and the prevalence is even higher in patients with DM who are ≥60 years old Prevalence of DM in hospitalized patients with HF HF cohorts, including both HF with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF), the prevalence of DM ranges from 10% to 47%. The prevalence of DM is higher in patients hospitalized with HF, with some reports of >40%. Risk factors of heart failure in DM - type 2 DM is considered as majour risk factor ( any patients with DM is considered as having stage A HF ) • Other risk factors associated with type 2 DM • Risk factors in non diabetic patients - hypertension - smoking - dyslipidemia , obesity - FH - IR , MS
Diagnosis Of newly diagnosed DM Of HF in diabetic patients
Treatment 1- Treatment goal 2- treatment target 3- treatment types ; A- Non pharmacological ;
B- Pharmacological Classification of GLDs according to the beneficial effect in prevention and treatment of HF in Diabetic patients A- drug therapy that worsens HF; 1- insulin ; - increase insulin resistance - it cause weight gain - fluid retention Indicated in stage D HF 2- SU ; - increased risk of hypoglycemia and weight gain - it binds to second SUR (SUR2) is present on skeletal and cardiac muscle and, with stimulation of this receptor, the cardiac output and cardiac workload are increased.83, 84 Studies regarding HF have been conflicting, with an increased frequency of HF usually being seen with sulphonylureas when compared to metformin
3- Dipeptidyl-peptidase-4 (DPP-4) inhibitors ; - they did not increase the major adverse cardiovascular event - was associated with increased risk of HHF without an increase in CV death sit gliptin have shown an increase in HF ranging from 21% to 84%. The Linagliptin in the Carmelina trials did not show an increased risk of HHF, so this may not be a class effect. pathological basis for the increased frequency of HF? - they increase cyclic AMP in cardiomyocytes. This may lead to calcium overload in the myocardium, which may adversely affect cardiac function. - increase sympathetic nervous system activity which increases ventricular hypertrophy and increases the risk of arrhythmias. - myocardial fibrosis. DPP-4 inhibitors are therefore not recommended in patients with HF, stage B, C and D. 4- Thiazolidinedione ; Disadvantage ; - fluid retention - increased body weight Its not recommended in stage B, C , D heart failure
B- diabetic drug therapy with neutral effect on HF 1- Alpha glucosidase inhibitor - reduction in MI - it may reduce left ventricular dysfunction - It produce robust reduction in A1C 2- GLP1RA ; Benefit
Reduce the risk for hospital for HF by 11% Indication in HF ; Because of the effect of GLP-1RAs on multiple comorbidities, they should be used in patients with HF without any anticipation of improvement or deterioration in HFrEF.116 Further evaluation of GLP-1RAs in the treatment of HFpEF is indicated
C-Diabetic drug therapy that may prevent or ameliorate HF 1- Metformin ; - protection of HF newer data have shown that patients utilizing metformin do have a survival benefit in HF when compared to patients on other glucose-lowering regimens. Use of metformin is still contraindicated in patients with unstable or acute HF.118
2- SGLT2I ; - Benefit in heart failure ;
Other novel drugs ; 1- Dual GLP1 I and GIP ( Tirzepatide ) Benefit in type 2 DM with HF ; - induce weight loss, dose dependent reduction in BW of 15%, 19.5%, and 20.9% with 5-, 10-, and 15-milligram doses, respectively, at 72 weeks in non-diabetic obese patients -enhance hepatic lipid metabolism, -normalize systemic insulin sensitivity, and reduce or even reverse metabolic dysfunction. The US FDA approved tirzepatide as the first dual GLP-1 and GIP receptor agonist for the treatment of T2DM in 2022. - greater reduction glycated hemoglobin levels than semaglutide - does not increase the risk of HHF -The apparent advantage of reducing glycated hemoglobin and BW of tirzepatide over GLP-1 RA has the potential to impact the clinical management or prevention of HF • 2- Dual SGLT2 and SGLT1 I (Sotagliflazon ) - reduce upregulation of SGLT1 -reduce glucose and HbA1C - Prevent the development of HF in type 2 DM - Reduce CV mortality and HHF
3- Bromocriptine ; reduced fasting and postprandial glucose levels, corrected dyslipidemia, and improved cardiovascular outcomes bromocriptine treatment for 52 weeks resulted in a 39% reduction in CV death-inclusive composite CV endpoints, including myocardial infarction, stroke, hospitalized angina, HHF, coronary revascularization, and CV death 4- Imeglimin ; - reduce insulin secretion by the pancrease - inhance insulin sensitivity
Assessment of newly diagnosed Diabetic patients before treatments Types A- Clinical assessment ; - Age and duration of DM - Body weight by assessment of BMI, WC - Measurement of BP - Assessment of complication as HF or CRD B- Laboratory assessment - severity of hyperglycemia ( by measurement of HbA1C ) - Presence of autoantibodies ( to differentiate type 1 from type 2 DM) - Assessment for the presence of IR ( By HOMA-IR ) - Assessment for MAU and Egfr - ECHO ; for presence and classification of HF
STEPS FOR TREATMENT 1- Estimate the pathophysiology of HF in diabetic patients ; A - Reduction of obesity Prevalence of obesity in type 2 DM ( 90% ) , in type 1 ( 28%) , In heart failure ( HFpEF 84% ) Classification ; Pathogenesis - pathogenesis of type 2 DM in obese - Treatment of obesity in DM ; Treatment target ( 5-10% of the base line body weight )
treatment types ; Treatment benefit
B – Treatment of Hyperglycemia ; determine the optimal HbA1C target Indication of tight glycemic control in HF - for prevention of HF ( Stage A , B ) Any increase in HbA1C by 1 is associated with increase CV mortality by 11-16% Important of tight glycemic control for prevention of HF ( stage A , B) ; Chronic hyperglycemia through glycosylation of myocardial protein can cause myocardial protein cross linking leading to increase fibrosis and higher risk of HF
B - insulin resistance ; 1- Prevalence ; - prevalence of IR in type 2 DM with HF ( 45% ) - prevalence of IR in HF patients without DM ( 33-70% ) 2- Pathogenesis of HF in patients with IR 3- Treatment ; C- Hypertension D- dyslipidemia E- endothelial dysfunction ; - GLDs that improve endothelial dysfunction - SGLT2I , GLP1RA , METFORMIN E- Inflammation
2- select optimal antidiabetic drugs when life style and weight reduction fail to achieve optimal A1c target ; who to select ; -According to their safety profile
- According to their beneficial effect in all CV risk factors
Factors that should be considered when we choice GLDs A - According to their glycemic efficacy ; - very high ; ( Dulaglutide , Samaglutide , Liraglutide , insulin ) - High ( GLP1RA not mentioned above , SGLT2I , ) - Intermediate ( Metformin , DPPT4I ) Avoid drugs with high glycemic efficiency in ; - old age - those at risk for hypoglycemia - Stage C, D HF B- According to reducing body weight efficiency ; - Very high ( Samaglutide , Tirzepatide ) - High ( Dulaglutide , Liraglutide ) - Intermediate ( GLP1RA not mentioned above , SGLT2I , DPPT4I , Metformin )
C- According to their beneficial effect in reducing the risk of HF ( Primery prevention ) in stage A, B HF Comorbidities must be considered, especially atherosclerotic cardiovascular disease (ASCVD), heart failure (HF) and chronic kidney disease (CKD) which can increase mortality. Newer therapies have positive outcomes for people with diabetes and these comorbidities, thus reducing the long-term complications and associated personal and financial costs. With the increasing evidence of positive long-term outcomes independent of glycaemic control from the newer agents, the expert working group considered the place of sodium-glucose co-transporter-2 inhibitor (SGLT-2i*) and glucagon-like peptide 1 receptor agonist (GLP-1RA) in therapy, recommending their use in NHS Scotland, considering - increasing evidence of positive long-term outcomes independent of glycaemic control -incorporation of SGLT-2i and GLP-1RA into guidelines from the American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD)[3] and more recently NICE 28[2] -duration of time since publication -prescribing in frailty -licensed indication
1- SGLT2I ; Its only approved first line therapy particularly ( Dapagliflazon , Empagliflazon , canagliflazon ) indication - in newly diagnosed DM as first line therapy - if patients already on metformin add SGLT2I irrespective of glycemic control - if patients on SU or insulin add or replace with SGLT2I 2- GLP1RA ; indication ; - As first line therapy in obese type 2DM or if SGLT2I is C/I or cannot be tolerated - As second line therapy if glycemic target is not achieved with SGLT2I 3- Metformin ; - As first line therapy - second line if GLP1RA is C/I - As third line
3- DPPT4I Indicated only on stage A HF if patients is not on GLP1RA 4- TZD ; only indicated on stage A HF
For treatment of HF ; - SGLT2I - GLPIRA - Metformin