Download
1 / 1
10 likes | 220 Views
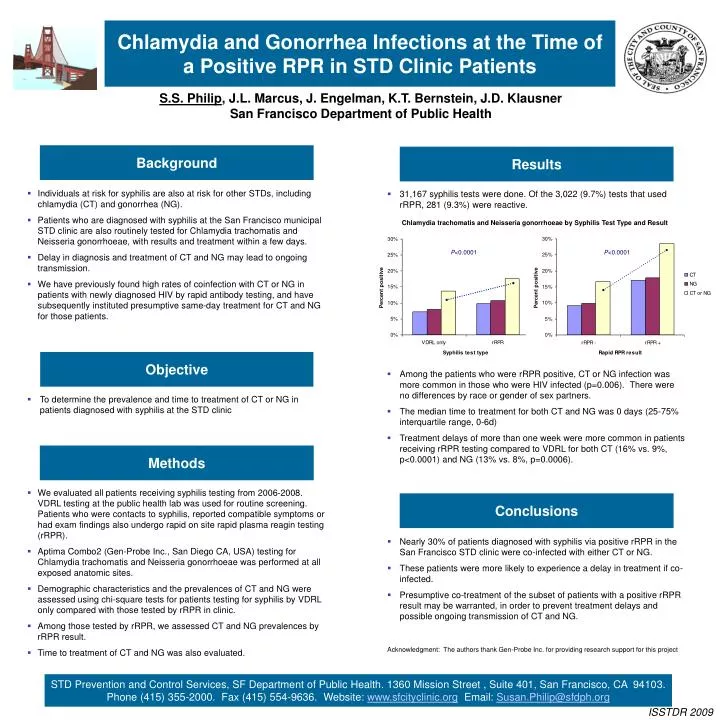
P <0.0001. P <0.0001. Chlamydia and Gonorrhea Infections at the Time of a Positive RPR in STD Clinic Patients. S.S. Philip , J.L. Marcus, J. Engelman, K.T. Bernstein, J.D. Klausner San Francisco Department of Public Health. Background. Results.

E N D
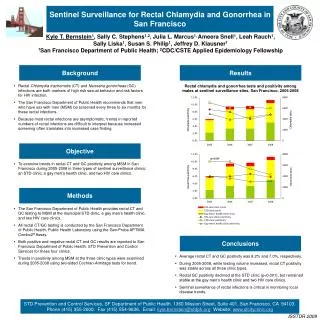
P<0.0001 P<0.0001 Chlamydia and Gonorrhea Infections at the Time of a Positive RPR in STD Clinic Patients S.S. Philip, J.L. Marcus, J. Engelman, K.T. Bernstein, J.D. Klausner San Francisco Department of Public Health Background Results • Individuals at risk for syphilis are also at risk for other STDs, including chlamydia (CT) and gonorrhea (NG). • Patients who are diagnosed with syphilis at the San Francisco municipal STD clinic are also routinely tested for Chlamydia trachomatis and Neisseria gonorrhoeae, with results and treatment within a few days. • Delay in diagnosis and treatment of CT and NG may lead to ongoing transmission. • We have previously found high rates of coinfection with CT or NG in patients with newly diagnosed HIV by rapid antibody testing, and have subsequently instituted presumptive same-day treatment for CT and NG for those patients. • 31,167 syphilis tests were done. Of the 3,022 (9.7%) tests that used rRPR, 281 (9.3%) were reactive. Chlamydia trachomatis and Neisseria gonorrhoeae by Syphilis Test Type and Result Objective • Among the patients who were rRPR positive, CT or NG infection was more common in those who were HIV infected (p=0.006). There were no differences by race or gender of sex partners. • The median time to treatment for both CT and NG was 0 days (25-75% interquartile range, 0-6d) • Treatment delays of more than one week were more common in patients receiving rRPR testing compared to VDRL for both CT (16% vs. 9%, p<0.0001) and NG (13% vs. 8%, p=0.0006). • To determine the prevalence and time to treatment of CT or NG in patients diagnosed with syphilis at the STD clinic Methods • We evaluated all patients receiving syphilis testing from 2006-2008. VDRL testing at the public health lab was used for routine screening. Patients who were contacts to syphilis, reported compatible symptoms or had exam findings also undergo rapid on site rapid plasma reagin testing (rRPR). • Aptima Combo2 (Gen-Probe Inc., San Diego CA, USA) testing for Chlamydia trachomatis and Neisseria gonorrhoeae was performed at all exposed anatomic sites. • Demographic characteristics and the prevalences of CT and NG were assessed using chi-square tests for patients testing for syphilis by VDRL only compared with those tested by rRPR in clinic. • Among those tested by rRPR, we assessed CT and NG prevalences by rRPR result. • Time to treatment of CT and NG was also evaluated. Conclusions • Nearly 30% of patients diagnosed with syphilis via positive rRPR in the San Francisco STD clinic were co-infected with either CT or NG. • These patients were more likely to experience a delay in treatment if co-infected. • Presumptive co-treatment of the subset of patients with a positive rRPR result may be warranted, in order to prevent treatment delays and possible ongoing transmission of CT and NG. Acknowledgment: The authors thank Gen-Probe Inc. for providing research support for this project STD Prevention and Control Services, SF Department of Public Health. 1360 Mission Street , Suite 401, San Francisco, CA 94103. Phone (415) 355-2000. Fax (415) 554-9636. Website: www.sfcityclinic.org Email: Susan.Philip@sfdph.org ISSTDR 2009 STD Prevention and Control Services, SF Department of Public Health, 1360 Mission Street , Suite 401, San Francisco, CA 94103. Phone (415) 355-2000. Fax (415) 554-9636. Website: www.sfcityclinic.org ISSTDR 2005