Download
1 / 16

E N D
1. Uveitis Aileen Dillon, M.D.
TPMG, Rheumatology
San Francisco
2. Uveal Tract
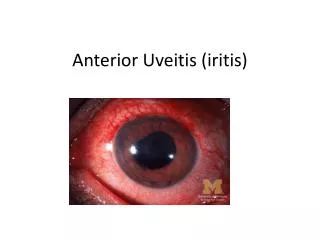
3. Uveitis Classification AU - Anterior Uveitis
Involves Iris &/or Pars Plicata
Includes Iritis, Ant Cyclitis, Iridocyclitis
IU - Intermediate Uveitis
Involves Pars Plana &/or adjacent Retina
Includes Pars Planitis, Post Cyclitis, Hyalitis, Basal Chorioretinitis
PU - Posterior Uveitis
Involves Choroid &/or Retina
Includes Focal, Multifocal, Diffuse Choroiditis, Chorioretinitis, Retinochoroiditis, Neuroretinitis
Panuveitis involves - 2 of 3 above
4. Uveitis General Facts Occurs worldwide
Incidence: 17 - 22.6 per 100,000/year
Prevalence: 38 -370 per 100,000
Accounts for 10-15% severe visual loss in US
Mean age at presentation = 40 yrs (IU -30 yrs)
Peak age of onset = 3rd & 4th decades
Systemic disease present in 50% (tertiary referral center)
5. Uveitis General Facts Chronic uveitis more common than acute or recurrent
Chronic uveitis most common form with IU
Non-granulomatous > granulomatous especially in AU
Non-infectious > infectious especially in PanU and AU
Bilateral > unilateral in PanU and IU
Bilateral = unilateral in AU and PU
6. Uveitis Distribution & Etiology Differs based on geography, genetics, environmental factors
Differs between community and tertiary referral practices
MEEI (tertiary referral 1237 patients) 1997
AU = 52%, IU = 13%, PU = 19%, PanU = 16%
LA (community (C) and tertiary (T) 426 patients) 1996
C: AU = 91%, IU = 1%, PU = 5%, PanU = 1%
T: AU = 61%, IU = 12%, PU = 15%, PanU = 9%
7. Causes of Anterior Uveitis (MEEI) Idiopathic 37.8%
HLA-B27 assoc arthropathies 21.6%
JRA 10.8%
Herpetic Uveitis 9.7%
Sarcoidosis 5.9%
Fuchs' heterochromic iridocyclitis 5%
SLE 3.3%
Others: lens induced (1.2%), Posner-Schlossman syndrome (0.9%), RA (0.9%), Syphilis, TB, phacogenic uveitis, Lyme disease, Wegeners, PAN, Relapsing Polychondritis
8. Causes of Intermediate Uveitis (MEEI) Idiopathic 69.1%
Sarcoidosis 22.2%
Multiple Sclerosis 8%
Lyme disease 0.6%
9. Causes of Posterior Uveitis (MEEI) Toxoplasmosis 24.6%
CMV retinitis 11.6%
SLE 7.9%
Birdshot retinochoroidopathy 7.9%
Sarcoidosis 7.5%
Acute retinal necrosis syndrome 5.5%
EBV retinochoroiditis 2.9%
Bechet's disease 2%
Others: Syphilis (2%), Toxocariasis, MS, Temporal Arteritis, POHS
10. Causes of Panuveitis (MEEI) Idiopathic 22.2%
Sarcoidosis 14.1%
Multifocal choroiditis and panuveitis 12.1%
Bechet's disease 11.6%
SLE 9.1%
Syphilis 5.5%
Vogt-Koyanagi-Harada syndrome 5.5%
HLA-B27 associated 4.5%
Others: Sympathetic Ophthalmia (4%), TB (2%), fungal retinitis (2%), bacterial panophthalmitis, lymphoma, RP, PAN, leprosy, DM, PSS
11. Uveitis Pathogenesis Immune privilege and the eye
Th1 cell mediated immune disease
APCs: retinal endothelial, Muller, ciliary epithelial, retinal pigment epithelial cells
Genetic associations:
acute anterior uveitis - HLA-B27
JRA iridocyclitis - HLA-DR5
Bechet's disease - HLA-B51
Birdshot chorioretinitis - HLA-A29
VKH - HLA-DR4
Pars Planitis & MS - HLA-DR15
12. Uveitis Animal Models (1 of 2)
13. Uveitis Animal Models (2 of 2)
14. Uveitis Diagnostic Approach Combined Ophthalmologic and Rheumatologic approach
Ophthalmologic patterns based on anatomic location, laterality, course, predominant morphology of posterior pole involvement
Appropriate physical examination
Selected tests:
Xrays: CXR (Sarcoidosis, TB), SI joints
Serologies: Toxo, Lyme, ANA, RPR, HLA
GI evaluation (IBD)
Lumbar Puncture (VKH)
Aqueous Humor analysis
15. Uveitis Complications Glaucoma
Cataracts
Cystoid macular edema (major cause of blindness)
Macular scar
Retinal detachment
Vitreous hemorrhage
Band keratopathy (JRA)
16. Uveitis Aileen Dillon, M.D.
TPMG, Rheumatology
San Francisco