Download
1 / 20
250 likes | 1.17k Views
Clopidogrel (Plavix) By Oksana Ekkert. Objectives . At the end of this presentation, participants should be able to: Describe CYP2C19 enzyme function and its variant alleles. Describe how CYP2C19 polymorphism affects the metabolism of the drugs.

E N D
Objectives At the end of this presentation, participants should be able to: • Describe CYP2C19 enzyme function and its variant alleles. • Describe how CYP2C19 polymorphism affects the metabolism of the drugs. • Understand the mechanism of action and metabolism of clopidogrel. • Identify multiple factors involved in clopidogrel response variability. • Understand the importance and the nature of clopidogrel-PPI drug interaction.
The routes of elimination for the 200 drugs sold by prescription in the United States according to the RxList data listed in April 2008 1
CYP2C19 • CYP2C19 is primarily present in hepatic tissue, but a significant amount is also found in the gut wall, particularly the duodenum. • Protein of 490 amino acids. • Located in a densely packed region on chromosome 10 along with CYP2C8, 2C9, and 2C18 genes.
Variant Alleles • Extensive metabolism: CYP2C19*1/*1 • Intermediate metabolism: CYP2C19*1/*2 or *1/*3 • Poor metabolism: CYP2C19*2/*2, *2/*3 or *3/*3 (also *4,*5) • Ultrarapid: CYP2C19*17 /*17
Comparison of pro-drugs and active drugs and clinical consequences
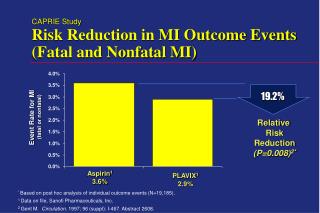
Clopidogrel • Anti-platelet agent • In 2005, world’s 2nd highest selling drug--U.S. sales $5.9 billion • Effective (with aspirin) for secondary prevention of MI and stroke, and thrombosis prevention after percutaneous coronary interventions (e.g., stent placement, angioplasty) • • Despite a short half-life ~2hrs, the irreversible binding of clopidogrel ’ s active metabolite to the platelet receptor leads to a prolonged pharmacodynamic effect.
OCH3 CH3 O O O C N HOOC N * HS Cl S 15% active metabolite Cl Gi Gs AC Clopidogrel ATP ADP P2X1 P2Y1 Gastro-intestinal absorption Gq G12 “Rho” Ca2+ flux Shape change PIP2 P2Y12 PLCβ Shape change + DAG IP3 Hepatic CYP Biotransformation PKC αi βγ Ca2+ mobilization MLCK-P AC PI3K 85% inactive metabolites (Esterases in blood) GP IIb/IIIa receptor activation Granule secretion PKB/Akt Rap1b GP IIb/IIIa receptor activation Initiation of Platelet Aggregation cAMP Stabilization of Platelet Aggregation VASP VASP-P PGE1 cAMP GP IIb/IIIa receptor activation Angiolillo DJ et al JACC 2007
T.E. Klein, J.T. Chang, M.K. Cho, K.L. Easton, R. Fergerson, M. Hewett, Z. Lin, Y. Liu, S. Liu, D.E. Oliver, D.L. Rubin, F. Shafa, J.M. Stuart and R.B. Altman, "Integrating Genotype and Phenotype Information: An Overview of the PharmGKB Project" (220k PDF), The Pharmacogenomics Journal (2001) 1, 167-170.
First oxidative step: conversion of clopidogrel to 2-oxo-clopidogrel • CYP1A2 (responsible for 36% of conversion): genetic polymorphisms: 16 identified SNPs • CYP2B6 (responsible for 19% of conversion): genetic polymorphisms: 29 identified SNPs • CYP2C19 (responsible for 45% of conversion): genetic polymorphisms: 25 identified SNPs Second oxidative step: conversion of 2-oxo-clopidogrel to the active metabolite • CYP2B6: responsible for 33% of conversion • CYP2C9 (responsible for 7% of conversion): genetic polymorphisms: 34 identified SNPs • CYP2C19: responsible for 20% of conversion • CYP3A4 (responsible for 40% of conversion): genetic polymorphisms: 20 identified SNPs
Not only CYP2C19 genetics, but-- • Genetics of CYP2C9*3 and ABCB1 have been shown to be important
Clopidogrel Response Variability20% do not have adequate response Intestinal Absorption Poor compliance Inadequate administration Variable absorption Genetic polymorphisms CYP2C19PMs, CYP2C9*3, ABCB1 Drug-drug interactions Genetic polymorphisms P2Y12 receptor Alternate pathways of platelet activation Genetic polymorphisms Hepatic Metabolism Cytochrome P450 pathway Active Metabolite P2Y12 Receptor (irreversible inhibition) GP IIb/IIIa receptor expression O’Donoghue M, Wiviott SD. Circulation. 2006;114:e600-e606 Simon T et al.NEJM. 2009;363-75 Feher G et al. Clin Genetics. 2009; 75:1-18.
Mechanisms of Clopidogrel Response Variability Limited absorption capacity with ceiling effect at 600mg loading dose7 Esterases85% ClopidogrelBisulfate Inactive Carboxylic Acid Metabolite Intestinal Absorption ? P-glycoprotein (MDR1 3435T genotype)2 15% CYP3A4 CYP3A5 CYP2C19 CYP2C9 CYP3A4 inducers: rifampin CYP3A4 inhibitors: erythromycin Hepatic P450 Cytochromes 2C19 Genetic polymorphisms 2C19 inhibitors 2C9*3 Genetic polymorphisms CYP1A2 CYP2B6, 2C19 Smoking (induction) Multistep Conversion Active Thiol Metabolite P2Y12 Receptor Inhibition of Platelet Aggregation (Wide Response Variability)1 1. Gurbel PA et al. Thromb Res. 2007;120:311-21. 2. Taubert et al. Clin Pharmacol. 2006;80:486-501. 3. von Beckerth et al. Eur Heart J.2007;28:1814-9.
Why do we need PPI’s with clopidogrel? Deepak LB, et al. Circulation 2008; 118:1894-1909
Ki (μM) values of PPI’s for CYP2C19 enzyme Li X, Andersson TB, Ahlstrom M, Weidolf L. Comparison of inhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole, lansoprazole, pantoprazole, and rabeprazole on human cytochrome p450 activities. Drug Metab Dispos. 2004 August 1;32(8):821-7.
Risk of All-Cause Mortality and Recurrent ACS in Patients Taking Clopidogrel and PPI Neither clopidogrel nor PPI PPI without clopidogrel Clopidogrel + PPI Clopidogrel without PPI 0.70 0.60 0.50 0.40 0.30 0.20 0.10 0 Proportion of Deaths or Recurrent ACS 90 180 270 360 450 540 630 720 810 900 990 1080 0 Days Since Discharge Ho PM, Maddox TM, Wang L, et al. JAMA. 2009;301(9):937-944.
Considerations for Healthcare Providers • Patients receiving clopidogrel for MI or stroke may not receive the expected antiplatelet activity if omeprazole is used concurrently. • Separating the time of administration of clopidogrel and omeprazole does not reduce the chance of the interaction. • The FDA does not have sufficient drug interaction information to provide recommendations for concurrent use of other PPIs. • There is no evidence that H2 antagonists (other than cimetidine) interfere with antiplatelet activity of clopidogrel. Both cimetidine and omeprazole are available in nonprescription (OTC) forms and patients should be educated to avoid these drugs if receiving clopidogrel. • Concurrent use of cimetidine, esomeprazole, etravirine, erythromycin, felbamate, fluconazole, fluvoxamine, fluoxetine, ketoconazole, voriconazole and ticlopidine should also be avoided because they may also reduce clopidogrel’s antiplatelet activity. • Rifampin has been shown to increase the concentrations of active metabolite through CYP3A4 induction. • At high concentrations in vitro, clopidogrel inhibits P450 (2C9). Accordingly, clopidogrel may interfere with the metabolism of phenytoin, tamoxifen, tolbutamide, warfarin, torsemide, fluvastatin, and many non-steroidal anti-inflammatory agents, but there are no data with which to predict the magnitude of these interactions. Caution should be used when any of these drugs is coadministered with clopidogrel.
In Conclusion The totality of all of the CYP2C19 polymorphism data suggests that it would be appropriate to begin genotyping all potential patients and thus identify those patients who would be at increased risk for thrombosis or bleeding if treated with clopidogrel.
References • Wienkers LC, Heath TG (2005) Nat Rev Drug Discov 4:825–833 (top 200) • S. R. Steinhubl. Genotyping, Clopidogrel Metabolism, and the Search for the Therapeutic Window of Thienopyridines Circulation February 2, 2010 121:481-483 • Plavix prescribing information. http://products.sanofi-aventis.us/plavix/plavix.html. Accessed February 20, 2010. • Kazui M, Nishiya Y, Ishizuka T, Hagihara K, Farid NA, Okazaki O, Ikeda T, Kurihara A. Identification of the human cytochrome P450 enzymes involved in the two oxidative steps in the bioactivation of clopidogrel to its pharmacologically active metabolite. Drug Metab Dispos. 2010;38:92–99. • Sibbing D, Koch W, Gebhardt D, Schuster T, Braun S, Stegherr J, Morath T, Schomig A, Kastrati A. Cytochrome 2C19*17 allelic variant, platelet aggregation, bleeding events, and stent thrombosis in clopidogrel-treated patients with coronary stent placement. Circulation. 2010;121:512–518. • Klotz U, Schwab M, Treiber G. CYP2C19 polymorphism and proton pump inhibitors. Basic Clin Pharmacol Toxicol 2004; 95: 2–8. • Beckerath N, Taubert D, Pogatsa-Murray G, et al. Absorption, metabolization, and antiplatelet effects of 300-, 600-, and 900-mg loading doses of clopidogrel: results of the ISAR-CHOICE Trial. Circulation 2005;112:2946-50 • Li X, Andersson TB, Ahlstrom M, Weidolf L. Comparison of inhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole, lansoprazole, pantoprazole, and rabeprazole on human cytochrome p450 activities. Drug Metab Dispos. 2004 August 1;32(8):821-7.