Download
1 / 39
400 likes | 820 Views
Optimizing Patient Radiation Dose. John Aldrich PhD FCCPM Department of Radiology Vancouver Coastal Health University of British Columbia. Outline. Changes in Medical Imaging Dose, Effective Dose and Risk Medical Imaging Utilization Status of Patient Dose in BC Skin Doses Summary.

E N D
Optimizing Patient Radiation Dose John Aldrich PhD FCCPM Department of Radiology Vancouver Coastal Health University of British Columbia
Outline • Changes in Medical Imaging • Dose, Effective Dose and Risk • Medical Imaging Utilization • Status of Patient Dose in BC • Skin Doses • Summary
Radiology • The use of x-rays in medical imaging has shown rapid growth in the last 10 years • This has been due to • Shorter imaging times • Increased indications for use • This has increased concern over the associated radiation dose to patients
Exam Type and Patient Dose at VGH Over the 11 year period the average dose to patients almost doubled Aldrich et al. CARJ 2005;56:94-99
Benefit and Risk • In all medical interventions there is a balance between benefit and risk • In the vast majority of cases the benefit from diagnostic x-ray studies far outweighs any detriment
D E What do we mean by Dose? Surface Dose (mGy) The surface dose of interest is normally the dose to skin Effective Dose (mSv) Effective dose takes into account the radiation sensitivity of different organs. External Radiation Surface Dose mGy E Effective Dose mSv
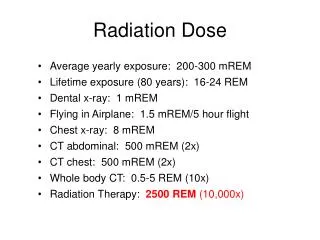
Patient Dose • The risk from radiation is measured by Effective Dose, a quantity which combines the radiation dose to the organs irradiated and their radiation sensitivities. • Common unit is the millisievert - mSv • Background radiation in Canada is 2 mSv per year • Risk of a lethal cancer is 1 in 20,000 per mSv ICRP (2008) Report 103
30 25 20 15 10 5 0 0 30 20 70 60 10 50 40 Age and Cancer Mortality Risk 1996 Re-analysis female Lifetime mortality risk per 100,000 per mSv) ICRP 60 average male Age at time of exposure
ACR Recommendations 2007 • Wider dissemination of Referral Guidelines • Routine monitoring of patient doses and optimization where necessary • Improved education regarding radiation dose from x-ray procedures for all staff involved in or using diagnostic imaging American College of Radiology J Am Coll Radiol 2007;4:272-284
A useful study is one in which the result will alter management or add confidence to the clinician’s diagnosis It is thought that about 15% of studies are not useful CAR - Referral Guidelines in Diagnostic Imaging (2005) Referral Guidelines
The chief causes of the wasteful use of radiology are: Repeating investigations which have already been done Investigation when results are unlikely to affect patient management Investigating too often Doing the wrong investigation Failing to provide appropriate clinical information and questions Referral Guidelines
Patient Dose in BC • In the past we have not continuously monitored patient dose • ‘Snapshots’ have been taken of the situation • In BC we estimated doses from CT in 2004 • At VGH we estimated CR and DR doses in 2004 • In VCHA we estimated CR doses in 2007
Optimum Dose • The 'optimum dose' is the minimum dose that provides the required diagnostic accuracy. • However, this is difficult to determine • A simpler first approach is to determine what doses are clearly TOO HIGH • Then a Reference Dose or Reference Level is normally set at the 75th percentile.
BC CT Dose Survey 2004 • Hospitals around BC were asked to provide data on routine head, chest, abdomen, and pelvis CT • Patient age, weight, slice width, number of slices, kVp, mA, CTDIvol, DLP • Data was collected from 18 hospitals
Summary - BC CT Survey 2004 Aldrich et al CARJ 2006;57:281
Diagnostic Reference Levels Dose-length product (DLP) is the ‘dose’ reported on each CT scanner for each patient *75% DLP values mGy.cm for a 70 kg patient
Predicted and Actual mA Decrease noise Increase noise Increase dose Decrease dose Aldrich J et al CARJ 2006 57:347
l1 l2 Computed Radiography(CR) x-ray image Cassette - based system using a storage phosphor instead of film-screens Exposure Latent Image Readout Erase
CR Relative Light Emission AEC Centre Cell Optimized Level
Patient Dose Monitoring It is now technically possible to estimate patient dose from most x-ray systems Both DLP and DAP values are directly related to patient dose
Dose Area Product Meter Collimator X-ray field Dose Area Product meter intercepts all radiation produced X-ray Tube
Practical Measurement • Meter records patient dose for the whole procedure • Record these values rather than fluoroscopy time • Newer units record DAP and Skin Dose Dual display of skin dose and effective dose during fluoroscopy/angiography
Skin Doses • During the 1990s there were many reported injuries to patients following fluoroscopy • High doses to the skin of the patient can cause erythema and even hair loss • This only occurs during long interventional angiographic procedures • The threshold for these effects is about 2000 mGy to the skin
Angiography Skin DosesPublished Data 1. Bor et al BJR 2004;77:315 2. McParland et al BJR 1998;71:175 3. Van de Putte et al BJR 2000;73:504
Skin Doses • It is essential that operators are correctly trained. • A course for physicians who use fluoroscopy is mandatory in VCHA and is now being implemented on the VCHA/FH/VIHA intranet • Skin dose should be monitored with a DAP meter, so that patients can be counselled if necessary
Summary - Referring Physicians • Avoid repeating investigations which have already been done • Choose the appropriate investigation • Provide appropriate clinical information and questions
Summary - Education • CAR Referral Guidelines should be made widely available • More information needs to be provided to users of diagnostic imaging on patient dose • Training course for physicians who use fluoroscopy
Summary– Purchasers and Managers • Monitor patient doses • CT DLP • Radiographic Rooms (DR, CR) DAP and EI • Fluoroscopy/Angiography DAP • Only purchase new equipment which incorporates patient dose estimation systems • Display dose indicators as overlays on PACS
Summary – Radiologists, Technologists • Review patient doses • Use Diagnostic Reference Levels for comparison • Optimize techniques based on this information • Relatively easy to reduce higher doses