Download

1 / 46
480 likes | 890 Views
Challenges in the Management of T2DM—Exploring the Role of GLP-1 Receptor Agonists: Southern Region. Frank Svec, MD, PhD Clinical Professor of Medicine Tulane University School of Medicine New Orleans, Louisiana Kevan Chambers Announcer Medscape Diabetes & Endocrinology.

E N D
Challenges in the Managementof T2DM—Exploring the Role of GLP-1 Receptor Agonists: Southern Region Frank Svec, MD, PhD Clinical Professor of Medicine Tulane University School of Medicine New Orleans, Louisiana Kevan Chambers Announcer Medscape Diabetes & Endocrinology
Challenges in the Managementof T2DM—Exploring the Role of GLP-1 Receptor Agonists: Southern Region • During today’s discussion, we will present 2 interactive questions • You may also submit a question at any time during the program by using the “Ask a Question” box in the lower right-hand corner of your screen • We hope to be able to answer at least some of your questions at the end of the program • There will be a brief assessment at the end of the program asking about the changes that you might make in your practice, on the basis of your participation today. Your responses will help us to improve the content of this and future educational programs
Frank Svec, MD, PhD Clinical Professor of Medicine Tulane University School of Medicine New Orleans, Louisiana
Ralph A. DeFronzo, MD Professor of Medicine Chief of Diabetes Division University of Texas Health Science Center at San Antonio San Antonio, Texas Staff Physician Department of Medicine Audie L. Murphy Division South Texas Veterans Health Care System San Antonio, Texas
Program Goal • Review the incidence and prevalence of type 2 diabetes mellitus (T2DM) • Evaluate evidence-based guidelines for the management of diabetes • Focus on the role of glucagon-like peptide (GLP)-1 receptor agonists to help you tailor therapies to your patients with T2DM
Age-Adjusted Percentage of US Adults With Diagnosed Diabetes 1994 1999 2008 <4.5% Missing Data 4.5-5.9% 6.0-7.4% 7.5-8.9% ≥9.0% Centers for Disease Control and Prevention: National Diabetes Surveillance System. http://www.cdc.gov/diabetes/statistics.
Incidence of T2DM • Approximately 20 million individuals with T2DM in the United Statesa • Additional 4-5 million individuals with undiagnosed diabetesa • 60 million individuals with prediabetes (ie, impaired glucose tolerance, impaired fasting glucose)b aCenters for Disease Control and Prevention. 2008. bNational Institute of Diabetes and Digestive and Kidney Diseases. 2008.
Obesity Trends* Among US Adults 1990 1999 2008 No Data 10–14% 15–19% <10% 20–24% 25–29% ≥30% *BMI ≥ 30 kg/m2, or about 30 lb overweight for 5’4” person. Centers for Disease Control and Prevention. 2008.
In your region, what percentage of your patients are obese? A. ≤ 25% B. 26%-50% C. 51%-75% D. ≥ 76%
49-year-old man with a 1-year history of T2DM Waiter in the French Quarter; 2 meals/day; weight conscious Father died of coronary disease; older brother has coronary disease Initial glycated hemoglobin (A1c) 9.1%; BMI = 29.5 kg/m2 Initial Presentation Case 1 • A1c today 8.1%; BMI = 28.8 kg/m2; LDL = 87 mg/dL; HDL = 33 mg/dL • Metformin 1000 mg twice daily and statin • Is concerned about heart disease; wants to lose weight; nervous about insulin
Cannot exercise 2 meals/day; snacks; drinks on the weekend Does not check blood glucose values at home BMI = 33.2 kg/m2; A1c 7.9%; LDL = 138 mg/dL; SCr = 1.6 mg/dL; blood pressure = 137/88 mm Hg ACE inhibitor/thiazide, sulfonylurea Case Presentations, Continued Case 2 • 67-year-old woman with a long history of T2DM • Cared for at Charity Hospital before Hurricane Katrina; moved to Mississippi; back to New Orleans • Old medical records lost • On insulin? • Lumbar disk disease and hypertension
T2DM Epidemic and Complications • 4000 new cases of diabetes are diagnosed daily • 800 deaths from individuals with T2DM daily • 200 individuals with T2DM experience an amputation daily • 50 individuals with T2DM develop blindness daily Rodgers G. http://www.nih.gov/news/radio/nov2009/20091110NDEP.htm
Ethnic Disparities • Highest incidence of diabetes among American Indiansa • High incidence of diabetes among Hispanics, Mexican Americans, and African Americansb,c • Lowest incidence of diabetes among whites aLee ET, et al. Diabetes Care. 2002;25:49-54. bCDC. MMWR Morb Mortal Wkly Rep. 2004;53:941-944. cAHRQ. http://www.ahrq.gov/research/diabdisp.htm.
Diabetes and Cardiovascular Disease • Increased incidence of atherosclerotic cardiovascular complicationsa • Incidence of myocardial infarction and stroke increaseda • High cost of managing micro- and macrovascular complicationsb aLotufo PA, et al. Arch Intern Med. 2001;161:242-247. bNational Institute of Diabetes and Digestive and Kidney Diseases. 2008.
Challenges to Diabetes Care • Complications among undiagnosed individuals with diabetes • Cost of medication • Patient propensity to lose weight
What is your greatest obstacle to initiating therapy with GLP-1 receptor agonists? A. Not being up-to-date on current safety and efficacy evidence supporting use of these agents in T2DM B. Cost of medication/insurance/managed care issues C. They offer no advantages over current antidiabetic agents D. Unfamiliarity with placement of this class within treatment guidelines E. Patients’ fear of injections or other patient-related factors
Reinforce positive results; his BMI went down Continue to reinforce the importance of diet and exercise GLP-1 agonist should be considered, given that his A1c is not at goal on metformin; he is worried about his heart, and wants to lose weight Need to check serum creatinine level and liver function Ask about history of pancreatitis Next Steps Case 1 49-year-old man with 1-year history of T2DM; on metformin; A1c, 8.1%; scared of insulin, worried about heart disease, and wants to lose more weight
0.0 -0.5 Change in A1c (%) -0.8% ± 0.1% -1.0 -1.1% ± 0.1% -1.5 0 10 20 30 40 50 60 70 80 90 Exenatide Sustained A1c Reductions Over 82 Weeks Mean Baseline A1c 82-Week Completer 8.3% 82-Week ITT 8.4% Open-label extension Placebo-controlled (All patients 10 mg BID) Time (week) Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447. 82-wk completer, N = 314; 82-wk ITT, N = 551; Mean ±SE. Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.
Durability of Exenatide: Weight Blonde L, et al. Diabetes Obes Metab. 2006;8:436-447.
Effects of GLP-1 Agonists on Cardiovascular Risk Factors • A subset achieved 3.5 years of exenatide exposure and had serum lipids available for analysis (n = 151) • Triglycerides decreased 12% (P = .0003) • Total cholesterol decreased 5% (P = .0007) • LDL-C decreased 6% (P < .0001) • HDL-C increased 24% (P < .0001) Klonoff DC, et al. Curr Med Res Opin. 2008;24:275-286.
Warn him about the potential gastrointestinal side effects of GLP-1 agonists (nausea, vomiting) and that they generally abate over time Educate on the need to control glucose and weight Review cardiovascular risk parameters Test blood glucose twice daily – before breakfast, before dinner DPP-4 inhibitors are a possibility, but they offer modest glucose lowering and are weight neutral Follow-up Case 1
American Diabetes Association • Lowering A1c to below or around 7% has been shown to reduce microvascular and macrovascular complications of T2DM American Diabetes Association. Diabetes Care. 2009;32(suppl1):S13-S61. Nathan DM, et al. Diabetes Care. 2006;29:1963-1972.
Lifestyle + MET + Intensive Insulin American Diabetes Association/European Association for the Study of Diabetes At diagnosis: Lifestyle + MET STEP 1 If A1c ≥7% Tier 2: Less-well-validated therapies* STEP 2 OR Tier 1: Well-validated core therapies* Lifestyle + MET + GLP-1 Agonist Lifestyle + MET + PIO Lifestyle + MET + SFU Lifestyle + MET + Basal Insulin Lifestyle + MET + Basal Insulin Lifestyle + MET + PIO + SFU STEP 3 MET = metformin; PIO = pioglitazone; SFU = sulfonylurea *Validation based on clinical trials and clinical judgment Adapted from: Nathan DM, et al. Diabetes Care. 2009;32:193-203.
American Association of Clinical Endocrinologists/American College of Endocrinology Rodbard HW, et al. Endocr Pract. 2009;15:540-559.
Pathophysiologic Approach to Treatment of T2DM Impaired Insulin Secretion TZDs GLP-1 analogues DPP-4 inhibitors Sulfonylureas Metformin Thiazolidinediones Thiazolidinediones Metformin _ Hyperglycemia Increased Hepatic Glucose Production Decreased Glucose Uptake DeFronzo RA. Diabetes. 2009;58:773-795.
Consensus Statements for T2DM • Consensus group of leading international endocrinologists and diabetologists with extensive clinical experience • Recent medical literature and all currently approved classes of medications should be considered • Common goal is to improve glucose control through individualization of therapy Nathan DM, et al. Diabetes Care. 2006;29:1963-1972. Nathan DM, et al. Diabetes Care. 2009;32:193-203.
GLP-1 Receptor Agonists • First-in-class exenatide approved in 2005 • Augment insulin secretion • Inhibit glucagon secretion • Lower fasting glucose and improve postprandial glucose profile Schnabel CA, et al. Vasc Health Risk Manag. 2006;2:69-77.
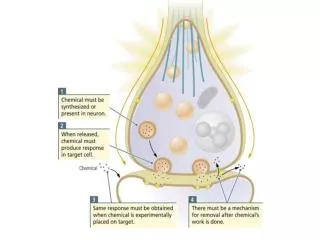
GLP-1 Actions in Peripheral Tissue Heart Neuroprotection Brain Appetite Stomach Stomach Gastric emptying Cardioprotection Cardiac output GI Tract GLP-1 _ Liver Insulin secretion β-cell neogenesis β-cell apoptosis Glucagon secretion + Glucose production Glucose Uptake Muscle Drucker DJ. Cell Metab. 2006;3:153-165.
Side Effects: GLP-1 Receptor Agonists and DPP-4 Inhibitors Davidson JA. Cleve Clin J Med. 2009;76(suppl5):S28-S38.
Side Effects: Metformin and Thiazolidinediones Seufert J, et al. Clin Ther. 2004;26:805-818.
Next Steps Case 2 67-year-old woman with a long history of T2DM; babysits grandchildren; on sulfonylurea; A1c, 7.9% • Emphasize the importance of exercise and diet • Serum creatinine is high, so cannot use metformin • Insulin is a common next step and may be considered, but associated with weight gain and hypoglycemia • GLP-1 agonists should be considered to help lower glucose levels and may be associated with mild improvements in blood pressure and lipid profile
Exenatide vs Insulin Glargine as Add-on Therapy in T2DM Exenatide group (n = 275) Insulin glargine group (n = 260) A1c Level (%) Change in Body Weight (kg) * * * * * * 0 2 4 8 12 18 26 Heine RJ, et al. Ann Intern Med. 2005;143:559-569.
Placebo BID Exenatide 5 μg BID Exenatide 10 μg BID Change in A1c Seen With Exenatide in Phase 3 Clinical Trials 0.2 0.1 0.1 METa MET + SFUc SFUb Change in A1c (%) -0.4* * -0.5* -0.6* - 0.8 -0.8* -0.8* -0.9* n 123 125 129 247 245 241 113 110 113 8.7 8.5 8.6 8.5 8.5 8.5 8.2 8.3 8.2 Baseline Mean (SE): *P < .005 aDeFronzo R, et al. Diabetes Care. 2005;28:1092-1100.bBuse JB, et al. Diabetes Care. 2004;27:2628-2635.cKendall D, et al. Diabetes Care. 2005;28:1083-1091. MET = metformin; SFU = sulfonylurea
Effects of Exenatide in Sulfonylurea-Treated Patients: Weight Buse JB, et al. Diabetes Care. 2004;27:2628-2635.
Illustrate the effects of binge alcohol consumption (hypoglycemia, pancreatitis risk) Another agent may help control hypertension A statin may help lower LDL Encourage home blood glucose monitoring DPP-4 inhibitors can be considered, but insulin may cause unwanted weight gain Follow-up Case 2
Medullary Thyroid Cancer and Pancreatitis • Liraglutide-induced medullary carcinoma is rare, but need to evaluate the patient’s risk • Increase in incidence of pancreatitis in patients with T2DM, but unclear whether it is associated with use of exenatide Parks M, et al. N Engl J Med. 2010;362:774-777.
Differences in Glycemic Control • Genetic variation on response to treatment commonly seen • Further studies are needed
Challenges in the Managementof T2DM—Exploring the Role of GLP-1 Receptor Agonists: Southern Region
Concluding Remarks • Treatment of diabetes requires consideration of multiple risk factors • Obesity/overweight is a prime factor in the development diabetes • Glucose control is important and can be accomplished without worsening adiposity • Discussion of side-effect profile of any medication ahead of time will enhance patient acceptance
Summary: T2DM Is 2 Diseases • Microvascular complications • Macrovascular complications • Two distinct pathogenic sequences • Two distinct clinical presentations
Thank you for participatingin this Regional CME activity.Please take a few moments to read the brief assessment to help us assess the effectiveness of this medical education activity.
Thank you for participatingin this Regional CME activity.To proceed to the online CME test, click on theEarn CME Creditlink on this page.