Download
1 / 15
160 likes | 473 Views
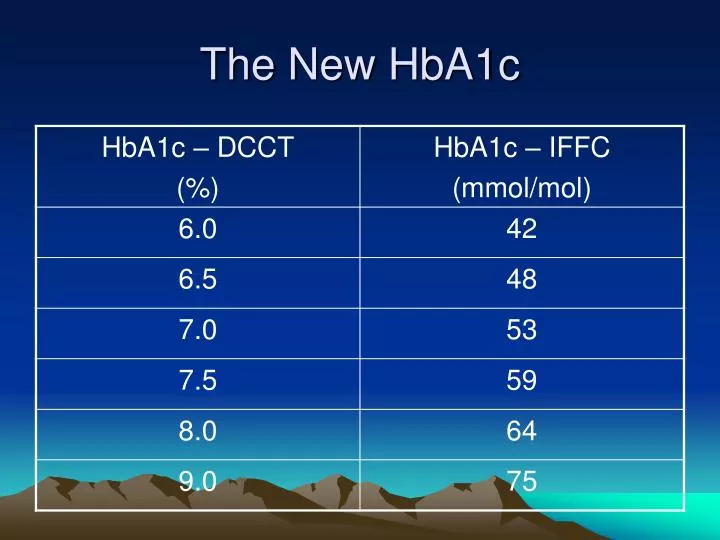
The New HbA1c. NICE Targets. HbA1c <6.5% BP <140/80 mmHg, but if kidney, eye or cerebrovascular disease <130/80 Lipids Cholesterol <4.0 mmol/l, LDL <2.0mmol/l Aspirin For all over 50 yrs and BP <145/90. Benefits of 10kg weight loss in Type 2 Diabetic.

E N D
NICE Targets • HbA1c <6.5% • BP <140/80 mmHg, but if kidney, eye or cerebrovascular disease <130/80 • Lipids Cholesterol <4.0 mmol/l, LDL <2.0mmol/l • Aspirin For all over 50 yrs and BP <145/90
Benefits of 10kg weight loss in Type 2 Diabetic • Fall of >30% diabetes related deaths • Fall of >50% fasting glucose • Fall of 10mmHg systolic BP • Fall of 20mmHg diastolic BP • Fall of 10% total cholesterol
Newer Agents for Glycaemic Control Thiazolidinediones Gliptins Incretin mimetics Insulins
Thiazolidinediones (pioglitazone, rosiglitazone) • They improve insulin-mediated glucose disposal by enhancing the sensitivity to insulin in the liver, adipose tissue and skeletal muscle. • Combination with biguanide or sulphonylurea or as triple therapy in the obese. • S/E Heart Failure. Increased fracture risk. Rarely liver toxicity (monitor LFT’s before treatment, and periodically thereafter). Hypoglycaemia. GI upset. weight gain.
Incretin Effect • Incretin hormones (GLP1 and GIP) produced by GI tract in response to nutrient entry. • Stimulates post-prandial secretion of insulin • Suppresses post-prandial secretion of glucogon (reduces gluconeogenesis) • Promotes satiety and reduces appetite.
Gliptins (Sitagliptin, Vildagliptin) • Inhibits the breakdown of incretins • Licensed for any triple therapy. And can be used with insulin. • Once daily tablet. (up to bd with vildagliptin) • More effective if used early in the course of diabetes. • Avoid if eGFR <50 • S/E Headache. URTI. Weight neutral. There are worries that it may also inhibit the breakdown of other peptide hormones involved in the immune system.
Incretin Mimetics (Exenatide and Liraglutide) • GLP 1 Analogue • It interacts with a specific receptor on the beta cell. • Helps weight loss • Sub cut injection (as rapidly degraded in the circulation) 60 minutes before meals. BD for exenatide, OD for Liraglutide
Incretin Mimetics 2 • Exenatide licensed triple therapy with sulphonylurea and metformin, Liraglutide triple therapy can also include a Glitazone. • NOT licensed for monotherapy. • NICE : HbA1c >7.5% and BMI > 35 in people of European decent or lower BMI (>30) if other ethnicity or weight loss would benefit other co-morbidities. • eGFR avoid if <30 exenatide, <60 Liraglutide. • S/E nausea very common. Hypoglycaemia more common if taken with a sulphonylurea. Acute pancreatitis.
Insulin in NIDDM • Newer synthetic insulin e.g insulin glargine (Lantus), and insulin determir (Glargine) • Reduced risk of hypoglycaemia due to ‘peakless’ profile • Very long acting • Can continue oral therapy • Titrated against fasting blood sugar • May ultimately need multiple injections, as for Type 1
Relevant Studies • UKPDS (Glyceamic control and hypertension) • DCCT (Glycaemic control) • EEDIT (Glycaemic control) • HOT (Hypertension) • ABCD (Hypertension) • ASCOT (ACEI) • HOPE (ACEI) • CARDS (Statins) • HPS (Statins) • HOT (Aspirin) although newer evidence suggests not.
Overt Hypothyroisim • Symptomatic • TSH <10 • Reduced serum free or total thyroxine
Sub-clinical Hypothyroidism • TSH 5-10 • Normal Thyroxine levels • Whether to treat is controversial • EXCEPT IN PREGNANCY or trying to conceive. • Risk of progression to overt is small (5% pa with antibodies, 2% pa without)
When to Treat • IF SYMPTOMS trial of thyroxine for 6 months, if feel better can continue (50%). • NO SYMPTOMS BUT ANTIBODIES not to treat but yearly surveillance.