Download
1 / 40
410 likes | 764 Views
Head Trauma. Artun KIRKER. MVA FALLING OF HEIGHTS VIOLENCE SPORTS PENETRATING WOUNDS INDUSTRIAL AND DOMESTIC ACCIDENTS One of the most frequent cause of death and disability in young adults. LOC:Loss of consciousness PTA:Post traumatic amnesia. Clinical manifestations.

E N D
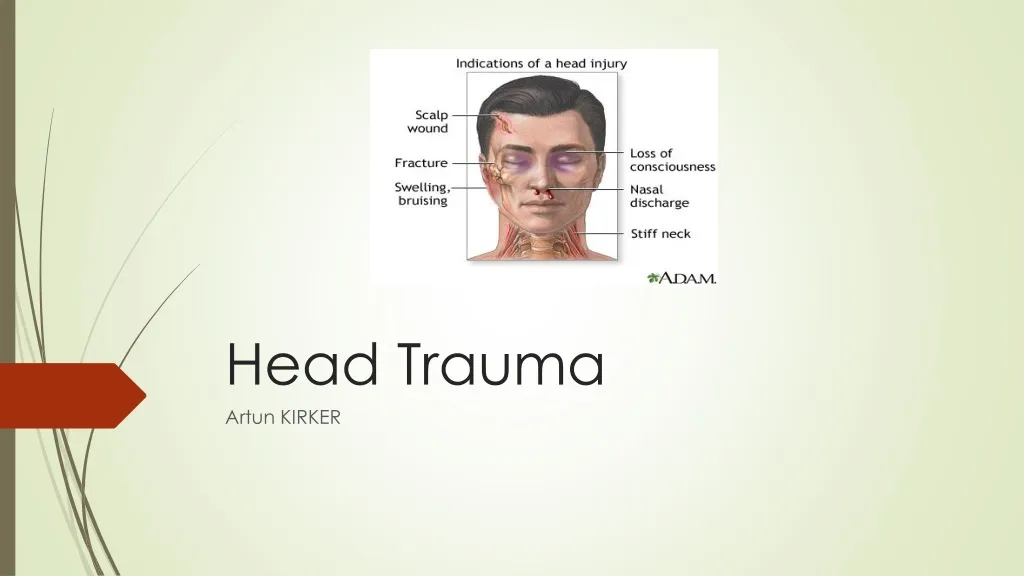
HeadTrauma Artun KIRKER
MVA • FALLING OF HEIGHTS • VIOLENCE • SPORTS • PENETRATING WOUNDS • INDUSTRIAL AND DOMESTIC ACCIDENTS • One of themostfrequentcause of deathanddisability in youngadults
Clinicalmanifestations • Bilateralpreorbitalecchymosis(Racooneyes) • Ecchymosis of themastoidprocess(Battle sign) • CSF rhinorrheaorotorrhea (Ear) • Cranialnervepalsy • Bleeding • Amnesia • Loss of consciousness • Cushingreflex—HT,Bradycardia,irregularrespirations
EpiduralHematoma • Between dura andskull • %1 of headtraumaaddmissions • %80 temporalarea • Middlemeningealartery is themostcommonsource • Dural sinusesandbridgingveinsmay be thesource • Moslyaffectsyoungadults
Clinical Mani. • Brief LOC • Lucidinterval(TALK AND DIE) • İpsilateraldilatepupil • Contralateralhemiparesis
Treatment • Conservative: if GCS>8,no midlineshiftand <30 ml blood • Surgery: Anisocoriaand GCS <8 • Best prognosticfactor is consciousness
SubduralHematoma • Collection of bloodbetween dura andaracnoid • Mva,falls (Severe trauma) mostlyforyoungs • Anticoagulants can be thecause in elderly • Acute <72h--hyperdense on CT Subacute 3-7 daysaftertrauma Chronic >3 weeks--hypodense on CT • Mostly in temporalandfrontalareas • High mortality&morbility
Clinicalpresent • Comaaftertrauma • Hemiparesis • increased ICP • Alteredlevel of consciousness • Acute form maypresentwith <9 GCS
Subarachnoidhemorrhage is extravasation of bloodintothesubarachnoidspacebetweenthepialandarachnoidmembranes
Symptoms • Headache (48%) • Dizziness (10%) • Orbitalpain (7%) • Diplopia (4%) • Visual loss (4%)
Signs • Mildtomoderate BP elevation • Temperatureelevation • Tachycardia • Papilledema • Retinalhemorrhage • Global orfocalneurologicabnormalities
Clinicalpresentation • Suddenonset of severe headache (worstheadache) • Accompanyingnauseaorvomiting • Symptoms of meningealirritation (%80 maytakeseveralhours) • Photophobiaandvisualchanges • Focalneurologicdeficits (CN III, CN VI--ICP) • Seizuresduringtheacutephase (Sudden ICP increase)
Stronglyassociatedwith SAH • Aged 40 yearsorolder • Witnessedloss of consciousness • Complaint of neckpainorstiffness • Onset of manifestationswithexertion • Arrivalbyambulance • Vomiting • Diastolicbloodpressure ≥100 mm Hg orsystolicbloodpressure ≥160 mm Hg
ClinicalGradingScales • Glasgow ComaScore--Clinical • TheFisherscale—CT Based • TheHuntandHessgradingsystem
TheFisherscale (CT scanappearance) is as follows: • Group 1 - No blooddetected • Group 2 - Diffusedeposition of subarachnoidblood, noclots, andnolayers of bloodgreaterthan 1 mm • Group 3 - Localizedclotsand/orverticallayers of blood 1 mm orgreater in thickness • Group 4 - Diffuseornosubarachnoidblood, but intracerebralorintraventricularclotsarepresent
Complications • Hydrocephalus (%20) • Rebleeding (HT,Anxiety) • Vasospasm (Delayedischemiafromarterialsmoothmusclecontraction of thelargecapacitancevessels at thebase of thebrain is theleadingcause of deathanddisabilityfollowinganeurysmal SAH) • Seizures • Cardiacdysfunction & pulmonaryedema
D.D • Aseptic Meningitis • Cluster Headache • Encephalitis • First Adult Seizure • HypertensiveEmergencies • Intracranial Hemorrhage • IschemicStroke • Meningitis • Migraine Headache • TransientIschemic Attack
DX • Noncontrast CT • LP (CT(-) andifsuspiciouscase):Mostsensitive but can be falsepositive—Traumatic tap • CTA,MRA,Catheterangio (toidentysource)
Work-up • EKG • CXR-Forevaluation of possiblepulmonarycomplications • Serum chemistry panel - Toestablish a baselinefordetection of futurecomplications • Complete bloodcount - Forevaluation of possibleinfectionorhematologicabnormality • Prothrombin time (PT) andactivatedpartialthromboplastin time (aPTT) - Forevaluation of possiblecoagulopathy • Blood typing/screening - Toprepareforpossibleintraoperativetransfusions • Cardiacenzymes - Forevaluation of possiblemyocardialischemia • Arterialbloodgas (ABG) - Necessary in patientswithpulmonarycompromise
Keep in mind • May be traumaticorspontaneous (Truma is morecommon) • Spontaneous SAH mostlycausedbyaneurysmalrupture • %30 occurs in sleep
Treatment-Emergency • ABC!--Intubation of patientswithcoma,depressedlevel of consciousnessorhigh ICP • Monitoring--Cardiacmonitoring • Pulseoximetry • Automatedand/orarterialbloodpressuremonitoring (arterial BP monitoring is indicated in high-grade SAH orwhenbloodpressure is labile) • End-tidalcarbondioxide, ifapplicable • Urineoutputviaplacement of a Foleycatheter
Thegoals of treatment in patientswithsubarachnoidhemorrhage (SAH) are as follows: • Blood pressurecontrol • Prevention of seizures • Management of intracranialpressure • Prevention of vasospasm • Control of pain • Maintenance of cerebralperfusion
Main goal is strictbloodpressurecontrol, withfluidrestrictionandantihypertensivetherapy • >130mm Hg MAP— I.V Beta blockers (Antihypertensive of choice) • High ICP orherniaton—intubation, hyperventilation, osmoticagents (mannitol) fordecrease ICP dramatically • Patientsmust be admittedtotheintensivecareunit • To minimize stimulithatmayleadto an elevation of ICP, havethepatientplaced in a darkened, quiet, privateroomandgivenmildsedationifagitated
Prevention of rebleeding (themostdreadedearlycomplication) is clippingtherupturedberryaneurysmorendovasculartreatment (ie, coiling)
Topreventvasospasmmaintenance of normovolemia, normothermia, and normal oxygenationareparamount • Oral nimodipine is themoststudiedcalciumchannelblockerforprevention of vasospasmafter SAH • Transluminalballoonangioplasty is recommendedfortreatment of vasospasmafterfailure of conventionaltherapy
Cerebralcontusions • Bruise of theneuralparenchyma • Causedbyinjurytosmallbloodvesselsmostly in thecrown of thegyrus • 4 types: Coup: Site of impact Counter coup: Opposite site of impact Gliding: parasagittalhaemorrhagiclesion (Rostraltocaudalmovement) Intermediary: in thedeepstructure of brain
Intracerebralhemorrhage • Causedbydecelerationinjury • Frontal—temporalregion %90 • May be delayedandwith SDH and SAH • Delayedtraumaticintracerebralhemorrhage:Presence of ICH in previously normal area of brain in initial CT—MORTALITY RATE GETS HIGHER
Treatment • Considernonsurgicalmanagementforpatientswith minimal neurologicaldeficitsorwithintracerebralhemorrhagevolumeslessthan 10 mL. • Admit ICU andmonitoringandserial CT scans
DiffuseAxonalInjury • Accelerating-deceleratinginjury • Confluenthaemorrhages • Frontal-temporal %80-90 • Axonsareinjuredbyshearingandimpaired transport • Is thecause of theloss of consciousness in headtraumapatients • CT is usually not enough • MRI T2W mayshowhyperintenselesions
Concussion • Clinicalterm—Post traumaticalteration of consciousness • Minimal ornochanges on CT/MR • Mild form of diffuseaxonalinjury





















