Download
1 / 42
430 likes | 770 Views
Monitoring colorectal Cancer after resection Relationship to operative curability. Prof. Fatma M. Nasrat Prof. Of Clinical Immunology Department of Clinical Pathology National Cancer Institute Cairo / Egypt. Follow-up after management of colon cancer with curative intent.

E N D
Monitoring colorectal Cancer after resection Relationship to operative curability Prof. Fatma M. Nasrat Prof. Of Clinical Immunology Department of Clinical Pathology National Cancer Institute Cairo / Egypt
Follow-up after management of colon cancer with curative intent. • Follow-up after definitive management has two primary goals. First, patients with a history of colorectal cancer are at higher risk than the general population for a second colon cancer primary. A colonoscopic screening may be of benefit in the early detection of a second primary malignancy or detection of a benign polyp, which can then be resected to potentially prevent the development of an invasive cancer. • Second, surveillance may increase the chance of identifying locoregional or distant recurrence that is potentially curable by surgery. It should be noted that it is this detection of potentially curable recurrent or second primary disease that justifies routine postoperative surveillance.
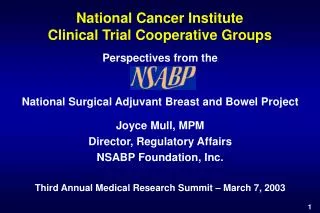
Time to Recurrence Proportion disease - free Months Modified Kaplan - Meier plot of disease – free survival of all patients
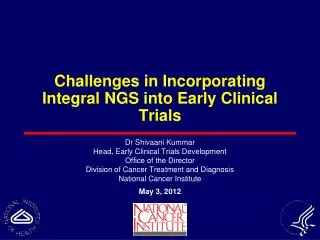
Proportion disease - free Modified Kaplan - Meier plot of recurrence at particular anatomic sites.
Guidelines for follow-Up care after primary treatment for colorectal cancer – American Society of Clinical Oncology * If they had stage II or III C.C. managed definitively.
Tests Not Recommended by ASCO for Regular Follow-up Care • Liver function tests. • Fecal occult blood test. • Computerized tomography ( CT ) scan. • Pelvic imaging. • Chest x-ray. • Complete blood count ( CBC ).
What is a “Tumor Marker” ? Biochemical indicators associated with the presence or progress of malignancy.
It is advisable to use the same CEA method consistently for a given patient because different CEA test methods do not give equivalent CEA test values for individual samples. • Only 50% to 60% of patients with colon carcinoma showed elevated blood CEA levels. • In cancer localized to the mucosa and submucosa, without invasion into the muscularis propria, the percentage of patients with an elevated test result falls to between 30% and 40%.
Levels higher than normal have also been found in Heavy smokers and in persons with cirrhosis, pancreatitis, Uremia, peptic ulcer, intestinal metaplasia of the stomach, as well as ulcerative colitis. The antigen has been reported in tissue of intestinal polyps: colonic inflammatory mucosa, and normal intestinal mucosa of children. The antigen is detected in about 50% of tumors of the breast, stomach, lung, and in other solid tumors.
The clinical usefulness of tumor markers can be assessed by determination of 1 - Sensitivity. 2 - Specificity. 3 - Positive predictive value. 4 – Negative predictive value.
Sensitivity • True Positives : The number of patients in a population with a positive test result for a tumor marker who actually have cancer. False Positives: The number of patients in a population with a positive test result for a tumor marker who do nothave cancer. Cut-off value : highest value obtained by the non- malignant groups ( normal persons and those with a benign disease ). Sensitivity = True positives ( positivity in disease) the abitity of a test to detect patients who actually have cancer.
Analytical vs Diagnostic Sensitivity. • Analytical sensitivity : minimum detectable concentration ( MDC) of an antigen that an immunoassay can reliably distinguish from “zero” concentration with 95% confidence. • Diagnostic sensitivity : proportion of individuals with disease who yield a positive test for antigen ) {I.e. TP / (TP + FN ) }. X 100
Specificity • True Negatives : the number of patients in a population with a negative test result for a tumor marker who do not have cancer. False Negatives : the number of patients in a population with a negative test result for a tumor marker who do have cancer. Specificity = true negative ( negative in health ) the ability of a test to distinguish those patients who do not have cancer from those who do .
Analytical vs Diagnostic Specificity • Analytical specificity : ability of an immunoassay to measure only the analyte of interest ( freedom from interferences); expressed typically as % cross- reactivity • Diagnostic specificity : Proportion of individuals without disease who yield a negative test for antigen { I.e. TN/(TN + FP)} . X 100
Positive Predictive Value ( PPV) : It is the probability that apatient with a positive test result actually has cancer.PPV,unlike NPV,markedly influenced by the prevelance of disease in the population tested. Negative Predictive Value (NPV) : It is the probabitity that a patient with a negative test result does not have cancer
HEALTHY & BENIGN DISEASE CUTOFF CANCER Ng/mL | | | | | | | | | | | | 0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 100.0 100% Specificity 100% Sensitivity Ideal Tumor Marker for Cancer
HEALTHY & BENIGN DISEASE CUTOFF CANCER | | | | | | | | | | | | 0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 100.0 20%FALSE NEG. 70%FALSE POS. Reality of Testing
Postoperative prognostic indicator Serial CEA in Monitoring Cancer therapy • Assessment of the adequacy of Surgical Removal of primary tumor. If the preoperatively elevated CEA level fails to decrease to normal range of 2.5 ng / mL or less within 4 to 8 weeks postoperatively, this strongly suggests persistent disease . Patients with a persistently elevated CEA level postoperatively may indicate an incomplete surgical resection or metastatic disease.
73% 18% 14%
CEA appeared the most accurate to identify patients with cancer following curative surgery
In this battery of tests, CEA was the first indication of disease recurrence . The lead time to detection of recurrence by serial CEA over all other diagnostic tests was between l and 18 months with a median of 3 months.
Indicator of asymptomatic recurrence • A persistent increase in the serum CEA concentration frequently indicate clinical evidence of recurrent disease . When an elevated CEA is detected in a patient in whom it was previously normal, the study should be repeated before a more extensive investigation . In one study in which 45 patients had false-positive values, 27 had an elevation in only one CEA value, which then returned to normal in the next several CEA determinations . Liver function test and renal function must be checked because abnormalities in either can elevate CEA level.
CEA may become elevated ( false positive value ) in patients undergoing adjuvant chemotherapy ( fluorouracil and levamisole ) without evidence of cancer recurrence, most likely because of the mild hepatic toxicity of these drugs. • No studies show a benefit to providing chemotherapy for an elevated CEA alone in the absence of measurable disease.
Routine Monitoring after Treatment • Evidence favoring routine monitoring. Advocates of CEA monitoring point to evidence that resection of isolated metastases, Particularly in the liver, increases survival compared with unresected patients or those with chemotherapy alone .If surgical intervention is potentially curative, any surveillance test that could detect a recurrence when the tumor is still resectable would be useful.
In a review of the patients who underwent surgical resection at the Mayo Clinic, there was a significant increase in survival for patients who had liver metastases detected because of an elevated serum CEA level or surveillance imaging test, when compared with those who had liver metastases detected by an elevation in liver function test, physical examination, or symptoms. In their multivariate analysis of factors affecting survival, CEA- detected disease was one of the strongest predictors of survival .
Therefore, the panel recommends serum CEA monitoring every 2 to 3 months for 2 years, only for those patients who would be willing and able to undergo a hepatic resection for recurrent disease.
Monitoring response to treatment for metastatic disease • Another potential role for CEA would be to aid clinical decision-making in patients with metastatic disease. Approximately 85 %of patients with metastatic colon cancer have an elevated CEA level.Several studies show that a decrease in CEA level while on chemotherapy, presumably indicating a tumor response, was associated with a better survival compared with patients whose CEA level did not decrease.
Therefore, a baseline value before treatment for metastatic disease is recommended, serial monitoring is appropriate every 2 to 3 months on active treatment if no other simple test is available to indicate a response. Two values above the baseline are adequate to document progressive disease and prompt the discontinuation of therapy, even in the absence of confirmatory radiologic testing .
Preoperative prognostic indicator • A preoperative CEA value predicts a higher rate of recurrence and colon cancer mortality compared with patients with normal levels .
In the National Surgical Adjuvant Breast Bowel Project ( NSABP) study of 945 patients, a preoperative CEA greater than 2.5 ng/mL increased the risk of recurrence by 1 to 2 fold in Dukes B patients ; if the preoperative CEA value was greater than 10 ng /mL,the risk was increased by 3.25 fold.Wanebo et al reported the time to recurrence was shorter if the CEA was elevated .13 versus 23 months for a CEA level greater than 5 ng/mL or less than 5 ng/mL,respectively : survival was higher in patients with CEA level less than 5 ng/mL.
A normal preoperative CEA level does not assure that CEA will remain normal.In a study by Zeng et al of 140 patients with normal preoperative CEA ( < 5 ng/mL ),32 developed a recurrence and 44% of these patients had a CEA level greater than 5 ng/mL at recurrence .
TPA TPA is a mixture of the low-molecular-weight epithelium associated cytokeratins, primarily cytokeratins 8,18, and 19. Released into the circulation during cell death (tumor necrosis ). Because cytokeratins are more abundant in cells undergoing mitosis and much less so in interphase cells, they are markers for cell proliferation. TPA is a sensitive but nonspecific markers for discriminating between progressive disease and disease in complete remission.
Stool DNA Because of the utility of identification of mutations in oncogenes and tumor-suppressor genes, it has been suggested that this observation may have a demonstrable advantage over occult blood determination .Some Studies have been reported which utilize purified DNA from stool samples in individuals known to harbor colorectal cancer and have detected these mutations .
Other markers Serum protein hexose Transferrin Ceruloplasmin
A rational postoperative surveillance program should include CEA measurements evry 3 to 6 months and a yearly. CT scan for the first 2 years. Colonoscopy can be performed every. 3 to 5 years after the resection. At the time of CEA measurement, a physician encountershould be scheduled in which the patients symptoms can be discussed and a physical examination performed. If a rising serum CEA level is detected on two consecutive measurements in the absence of imageable disease by CT scan, an FDG-PET scan can be considered .lesions found on colonoscopy should be managed appropriately either with colonoscopic resection or surgical management. These surveillance guidelines should allow for the early detection of recurrence or second primary, lesions and therefore provide the potential to impact patient to outcome.
There is a tremendous literatures on cancer, but what we know for sure about it can be printed on a calling card