Download

1 / 45
880 likes | 3.85k Views
Implant Types. SubperiostealPrimarly used to retain complete denture Transosteal.Mostly used to anchor complete denture EndostealPlaced within alveolus or basal bone. Endosteal Implants. Plate implants (Blades)Wedge shaped or rectangular in cross sectionGenerally 2.5 mm wide, 8-15bmm deep, 15-30 mm longOne stage, lower success rate, difficult placement, large in sizeCylindrical (Root Form)One stage and two stage3-6 mm wide, 8-20 mm long.

E N D
1. Implant-Supported Fixed Prostheses
Wael Al-Omari
3. Endosteal Implants Plate implants (Blades)
Wedge shaped or rectangular in cross section
Generally 2.5 mm wide, 8-15bmm deep, 15-30 mm long
One stage, lower success rate, difficult placement, large in size
Cylindrical (Root Form)
One stage and two stage
3-6 mm wide, 8-20 mm long
5. Cylinders (Root Form) Implants Advantages:
Suitable for multiple intraoral locations
Precise placement
Low adverse effects at incidence of failure
Predictable high success rate.
Available as threaded, non-threaded, coated and non-coated with hydroxyapatite, plasma sprayed, grit blasted, and acid etched
Made of titanium or titanium alloy
Gold standard (Branemark system: 92% success over 15 years
6. Treatment Planning Indications
Inability tom wear RPD or CD
Long span bridge with questionable prognosis
Unfavorable natural tooth abutments
Single missing tooth in an otherwise intact dentition
8. Treatment Planning Contraindications:
Acute or terminal illness
Uncontrolled metabolic diseases
Radiated site for previous cancer therapy
Pregnancy (elective procedure)
Poor motivation and poor oral hygiene
Lack of clinical and or technical expertise
Unrealistic patient�s expectations
9. Clinical Evaluation Visual inspection and palpation
Determine adequacy of bone
Relevant anatomic features
Flabby excess soft tissue
Bony ridges
Sharp osseous formations
Bony undercut
10. Radiographic Evaluation The best initial film in panoramic view.
Use small radio-opaque reference object to correct for magnification error (Ball bearing)
New panoramic radiography machines have standardized enlargement ratios.
Bone width in anterior mandible and maxilla assessed with cephalometric film
Location of inferior alveolar canal and maxillary sinus assessed with CT scans.
Bone width and bony undercut also assessed with CT scans
12. Diagnostic Casts Study remaining dentition
Evaluate the residual bone
Analyze maxillomandibular relationships.
Diagnostic wax up
Check proper fixture location, alignment, and relation to remaining teeth.
Surgical templates to guide surgical fixture installation.
13. Bone Sounding Used when results of radiographic and clinical examinations are inconclusive.
Sounding of the bone with a probe:
Under local anesthesia
Needle or sharp caliper pushed through the tissue until it contacts bone
14. Principles of Implant Location Anatomic limitations
Ideally, 10 mm of vertical bone and 6 mm of horizontal bone dimensions should be available.
Adequate space between adjacent implants: minimum of 3.0 mm
2.0 mm above superior aspect of inferior alveolar canal
5 mm anterior to mental foramen
1.0 mm from adjacent teeth.
15. Principles of Implant Location Anterior Maxilla:
1.0 mm between implant apex and nasal vestibule
Implants should be located slightly off midline on either side of incisal foramen.
Posterior Maxilla:
Poor bone quality, minimum of 6 months for osseointegration. One implant for every tooth
1.0 mm between implant apex and maxillary sinus floor.
16. Principles of Implant Location Anterior Mandible:
The most straightforward area for implant placement. Very good bone quality and quantity
Place implant through the entire bone depth to engage the cortex of inferior border of mandibular border, and 5.0 mm anterior to mental foramen.
Posterior Mandible:
2.0 mm above inferior alveolar canal
Use short implants and place more implants
Otherwise, nerve repositioning or non implant borne prosthesis
17. Restorative Considerations Implant Placement:
To avoid damage: 1.0 mm from adjacent tooth.
Oral Hygiene access: 3.0 mm between adjacent implants.
Proper implant angulation to position screw access lingually.
Long axis of implant positioned in the central fossae of restoration.
Optimal emergence profile: implant positioned
2-3 mm inferior to emergence position of the restoration
20. Surgical Guide A clear resin template made from diagnostic wax up
Objectives of surgical guide:
Delineate the embrasures
Locate the implant within the restoration contour
Align implant with the long axis of the restoration.
Identify the level of the emergence position from the soft tissue
22. Implant Surgery Surgical Access: crestal incision
Implant Placement:
Use low-speed, high-torque handpiece
Avoid overheating
Use series of gradually enlarged burs
Avoid any contamination for the implant.
Non-threaded implants are tapped into and threaded screwed into place.
Implant Evaluation
Implant Uncovering
23. Implant Restorations
24. Implant Restorations
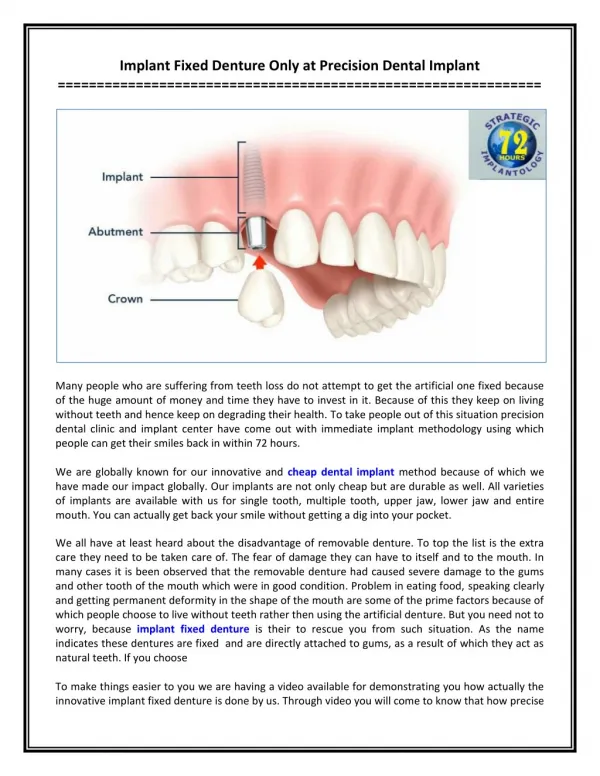
26. Implant Restorations Abutments
The component that screw directly into the
implant fixture.
In screw- retained model, abutments support the
restoration.
In cement retained approach, abutments are shaped like
conventional crown preparation.
Take many forms and angulations
Made of titanium or titanium alloy or all ceramic
Nonsegmented crowns: UCLA abutments
28. Implant Restorations Abutments:
Correct abutment size selection is based on:
Vertical distance between fixture base and opposing dentition.
Existing sulcular depth.
Esthetic requirements
29. Implant Restorations Impression Posts:
Transfer intraoral location of implant or abutment to a similar position on the laboratory
Fixture type and Abutment Type.
Direct (pick-up or open-tray impression technique)
Indirect (closed-tray impression technique)
Impression material could be addition silicone or polyether
Impression post is joined to laboratory analog
Multiple divergent implants: pick-up technique
32. Implant Restorations Laboratory Analogs
Represent exactly the top of the fixture or the abutment in the laboratory cast
Fixture analogs and abutment analogs.
Can be screwed into impression post before pouring.
Gingival tissues reproduced by injecting an elastomer around laboratory analog before pouring.
With fixture analog, abutment can be changed in the laboratory to correct implant angulation
33. Implant Restorations Waxing Sleeves
Could be attached to abutment on lab. Model
May also be directly concerted to implant body analog in nonsegmented implant crowns (UCLA abutments).
May be completely plastic patterns, or
combination of plastic and gold alloy cylinder
Prosthesis-retaining Screws
Made of titanium, titanium alloy or gold alloy
Can be tightened with screwdriver or wrench
Screws sunk in the crowns are covered with resilient material then sealed with composite
35. Implant Restorative Options Distal Extension Implant Restoration:
Implant-tooth born prosthesis
Fully implant-supported prosthesis
Two implants to support 3-unit bridge
Implant for each missing tooth
Long Edentulous Span:
Similar options.
If natural tooth connected to implant use telescopic crown to protect he tooth.
If soft and hard tissue missing consider use resin teeth an replace soft tissue with acrylic (Hybrid Restorations).
37. Implant Restorative Options Single Tooth Implant
Requires esthetics, antirotation, simplicity and variability.
Difficulty in matching the soft tissue contour of adjacent natural teeth
Fixed Restoration of Completely Edentulous Arch
Hybrid prosthesis: min. 5 implants in the mandible, and 6 implants in the maxilla
Metal ceramic Rehabilitation: esthetic only if minimum bone loss occurred
Avoid esthetic and poetic problems by avoiding placement of implants near the midline and restore maxilla incisor teeth with pontics
39. Implant Restorative Options Cement Retained Implant Crowns
Simplicity, economy, allows correction of minor angle correction, , replacement of small teeth. Antirotational features are necessary
Screw Retained Implant Crowns
Retrievable
Suffer from screw loosening
Screws should be sufficiently tightened.
Eliminate lateral forces and utilize antirotational features
41. Biomechanical Factors Occlusion
Direct forces n long axis.
Avoid long cantilevers.
Minimize lateral forces.
Place lateral forces as far anterior in
the arch as possible.
Connect implants.
Proper implant angulation.
Reduce occlusal table dimensions.
Increase the number of implants.
42. Biomechanical Factors Connecting Implants to Natural Teeth
Creates excessive forces due to differences in relative mobility
Problems include failure of osseointegration, cement failure, screw loosening, and failure of prosthetic components.
Solutions include, avoid connecting plant to natural teeth, telescopic coping on the natural tooth, stress breaking attachment
43. Biomechanical Factors Implant and Framework Fit
Lack of passive fit results in excessive compressive forces on the interfacial bone
Check passive fit with only one screw in place.
Non-passive fit: section and solder
Shock Absorbing Elements
Designed into implant system or occlusal surface of the restoration
Based only on theoretical calculations and their need is controversial.
44. Maintenance and Complications Follow-up, OHI, scaling, adjusting occlusion
Bone loss: > 0.2 mm/year is alarming
Bone loss of 25% to 30% necessitates revision surgery
Prosthetic failure