Download
1 / 31
310 likes | 841 Views
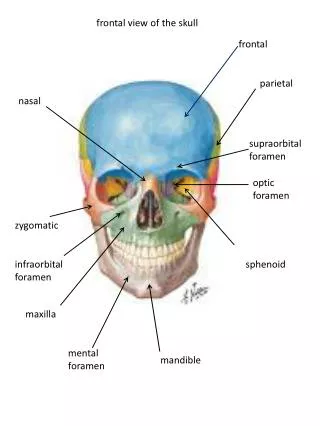
Anatomy. . EthmoidMaxillaPalatineLacrimalPterygoid plate of SphenoidNasal Inferior Turbinate. Bony Structure. Nose and Para nasal sinuses. Arterial Supply. External Carotid Maxillary A. SphenopalatineInternal Carotid Ophthalmic A. Ant. Ethmoid Post. Ethmoid Supraorbital Supratrochlear.

E N D
1. Nasal and sinus disease Babak saedi M.D
Assistant professor of Tehran university
2. Anatomy
4. Nose and Para nasal sinuses
6. The Nose Vascular Supply
- Anterior - branches of internal carotid
- Posterior - distal branches of external carotid
8. Facial Analysis Analysis of nose is very important
9. Facial Analysis Face: General
Divided in 1/3�s
trichion to NFA
NFA to subnasale
subnasale to menton
10. Function of Nose & Paranasal Sinuses Humidifying and warming inspired air
Regulation of intranasal pressure
Increasing surface area for olfaction
Lightening the skull
Resonance
Absorbing shock
Contribute to facial growth
12. Sinus Maxillary
Frontal
Ethmoid
Sphenoid
16. EpistaxisAnterior 90% (Little�s Area) Kisselbach�s plexus - usually children, young adults
Etiologies
Trauma, epistaxis digitorum
Winter Syndrome, Allergies
Irritants - cocaine, sprays
Pregnancy
17. EpistaxisPosterior 10% of all epistaxis - usually in the elderly
Etiologies
Coagulopathy
Atherosclerosis
Neoplasm
Hypertension (debatable)
18. EpistaxisManagement Pain meds, lower BP, calm patient
Prepare ! (gown, mask, suction, speculum, meds and packing ready)
Evacuate clots
Topical vasoconstrictor and anesthetic
Identify source
19. EpistaxisManagement Anterior Sites
- Pressure +/- cautery and/or tamponade
- all packs require antibiotic prophylaxis
20. Packing - anterior BIPP impregnated gauze in layers
21. EpistaxisPosterior Packing Need analgesia and sedation
require admission and 02 saturation monitoring
22. Packing - posterior Inflatable balloons
23. EpistaxisComplications severe bleeding
hypoxia, hypercarbia
sinusitis, otitis media
necrosis of the columella or nasal ala
24. Osler-Weber-Rendu
25. Scope of Sinusitis Affects 30-35 million persons/year
25 million office visits/year
Direct annual cost $2.4 billion and increasing
Added surgical costs: $1 billion
Third most common diagnosis for which antibiotics are prescribed
Third most common diagnosis for which antibiotics are prescribed. Rhinosinusitis, like asthma is becoming more prevalent.
McCraig LF, Hughes JM: Trends in antimicrobial drug prescribing among office based physicians in the US. JAMA 1995, 273:214-219Third most common diagnosis for which antibiotics are prescribed. Rhinosinusitis, like asthma is becoming more prevalent.
McCraig LF, Hughes JM: Trends in antimicrobial drug prescribing among office based physicians in the US. JAMA 1995, 273:214-219
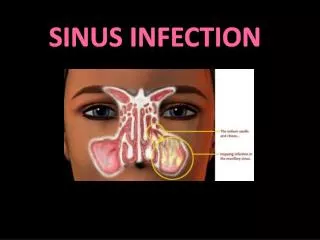
26. Sinusitis 4 paranasal sinuses, each lined with pseudostratified ciliated columnar epithelium and goblet cells
Frontal
Maxillary
Ethmoid
Sphenoid
27. Ostiomeatal Complex Ostiomeatal complex is that area under the middle meatus (airspace) into which the anterior ethmoid, frontal and maxillary sinuses drain
Posterior ethmoids drain into the upper meatus
Ostiomeatal complex is the functional relationship between the space and the ostia that drain into it
28. Viral Rhinosinusitis Most upper respiratory infections are viral
Short lived, last less than 10 days
Sinus mucosa as well as nasal mucosa is involved
Most will clear without antibiotics
Treatment: decongestants, nasal lavage, rest, fluids
29. Classification of Bacterial Sinusitis Acute bacterial sinusitis- infection lasting 4 weeks, symptoms resolve completely (children 30 days)
Subacute bacterial sinusitis- infection lasting between 4 to 12 weeks, yet resolves completely (children 30-90 days)
Chronic sinusitis- symptoms lasting more than 12 weeks (children >90 days)
Some guidelines add treatment failure + a positive imaging study
30. Differentiating Sinusitis from Rhinitis Sinusitis
Nasal congestion
Purulent rhinorrhea
Postnasal drip
Headache
Facial pain
Anosmia
Cough, fever
Rhinitis
Nasal congestion
Rhinorrhea clear
Runny nose
Itching, red eyes
Nasal crease
Seasonal symptoms
31. Pathogenesis of Nasal Obstruction Viral upper respiratory infections
Daycare centers
Allergic and nonallergic stimuli
Immunodeficiency disorders
Immunoglobulin deficiency (IgA, IgG)
Anatomic changes
Deviated septum, concha bullosa, polyps
32. Treatment of Acute Sinusitis Antihistamines recommended if allergy present
Oral or topical
Decongestants
Oral or topical
Antibiotic when indicated (bacteria)
Nasal irrigation
Guaifenesin 200-400 mg q4-6 hrs
Hydration
33. Antibiotics for Acute Bacterial Sinusitis Amoxicillin 500 mg tid for 10-14 days
First line choice in most areas
Local differences in antibiotic resistance occur
Where beta-lactamase resistance is an issue
Amoxicillin/clavulanate
Cefuroxime
Cefexim
Cefprozil
34. Additional Antibiotics for Acute Bacterial Sinusitis Amoxicillin should be considered because of its efficacy, low cost, side-effect profile, and narrow spectrum (45-90 mg/kg/d in children; 500 mg tid or qid in adults for 10 to 14 days)
If penicillin-allergic clarithromycin or azithromycin
Erythromycin does not provide adequate coverage
Trimethoprim/suflamethoxazole and erythro/sulfisoxazole have significant pneumococcal resistance Give prescription for antibiotic for 5 days, if no response switch to another, if responding refill for full 10 day course. Where co-pays are involved give entire 10 day prescription initially. Give prescription for antibiotic for 5 days, if no response switch to another, if responding refill for full 10 day course. Where co-pays are involved give entire 10 day prescription initially.
35. Rhinoscopy Aids in Diagnosing Nasal polyps
Septal deviation
Concha bullosa
Eustachian tube dysfunction
Causes of hoarseness
Adenoid hyperplasia
Tumors
36. Chronic Sinusitis Symptoms present longer than 8 weeks or 4/year in adults or 12 weeks or 6 episodes/year in children
Eosinophilic inflammation or chronic infection
Associated with positive CT scans
Poor (if any) response to antibiotics
37. Sx of Chronic Sinusitis Nasal discharge
Nasal congestion
Headache
Facial pain or pressure
Olfactory disturbance
Fever and halitosis
Cough (worse when lying down)
38. Bacteria Involved in Chronic Sinusitis Role of Viruses is Unknown Streptococcus pneumoniae
Haemophilus influenza
Moraxella catarrhalis
Staph aureus
Coagulase negative staphylococcus
Anerobic bacteria
Staph aureus, other streptococcal bacteria, pseudomonas, and E.coli are uncommon bacteria found in ABS.
Staph aureus, other streptococcal bacteria, pseudomonas, and E.coli are uncommon bacteria found in ABS.
39. CT Scan Maxillary and Ethmoid Sinuses
40. Sinusitis
41. Treatment of Chronic Sinusitis Nasal steroid spray
Guafenesin
Decongestants
Steam inhalation
Nasal irrigation
Antibiotics with exacerbations
42. FESS
43. Sinus endoscopy
47. Complications of Sinusitis Orbital
Diplopia, proptosis
Periorbital erythema, swelling
Bone
Periosteal abscesses
Brain
Intracranial abscesses causing neurologic symptoms
Cellulitis can spread around the eye and cheek indicated by swelling and erythema. Symptoms of meningitis, severe headache, focal neurologic symptoms signal spread to intracranial areas. Cellulitis can spread around the eye and cheek indicated by swelling and erythema. Symptoms of meningitis, severe headache, focal neurologic symptoms signal spread to intracranial areas.
48. Nasal obstruction Infection
Allergy
Adenoid hypertrophy
Nasoseptal deformity
Chronic sinusitis
Septal hematoma (abscess)
Foreign body
Neoplasm
Choanal atresia
49. Looking at the turbinates: Diagnosis?
50. Nasal Polyp
51. Septal deviation
52. Allergic Rhinitis