Download
1 / 26

E N D
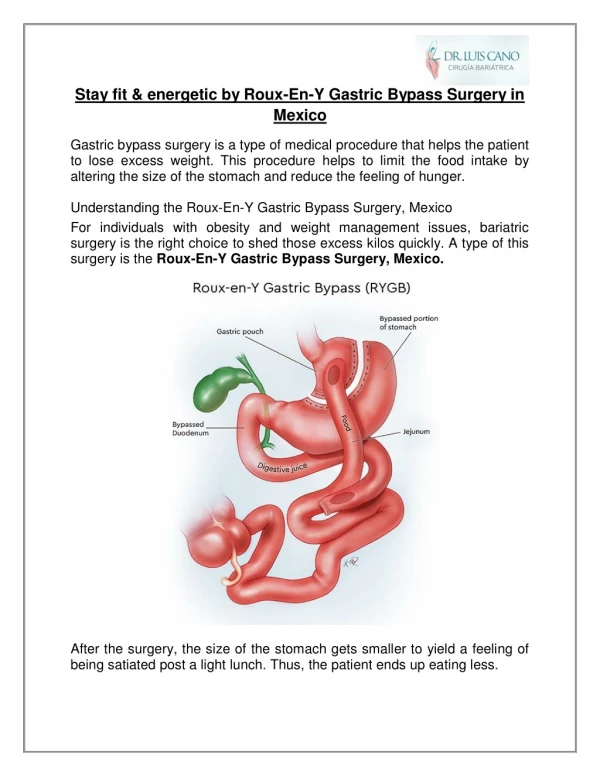
1. Roux-en-y procedure Ri ???
2007/9/24
4. Characteristics intrinsic aboral peristaltic propulsive action ? conductive, not a capacitance, tube
unidirectional aboral peristaltic action offers the property of a one-way valve ? reflux is prevented.
?exploited to allow esophagojejunal anastomosis and drainage of the biliary and pancreatie ducts.
?valuable means of draining cysts and fistulas.
5. jejunum transected and straightened, it can be extended to a greater distance from its vascular anchorage
the rapid clearance of the jejunal segment ensures that there is little absorption within it
6. Complications Wound infection
Intra-abdominal abscess
Leak/ Bleeding/ Stenosis
Internal hernia
Pulmonary embolism
9. Anemia, metabolic bone disease, nutritional deficiencies (iron, calcium, vitamin B12 and folate),
Gastric�ulcer can occur in 3% of the cases, but can be cured most often by drugs.
Stenosis of the anastomosis occurs in 5 to 7% of the cases, with vomiting, and can be cured by endoscopic dilatation.
Biliary tract stone
Late small bowel obstruction due to adhesions or an internal hernia
10. Postgastrectomy Syndrome Afferent and efferent loop syndrome
Dumping syndrome
Alkaline reflux gastritis
Nutritional disturbance
Retained antrum syndrome
Marginal ulcer
Postvagotomy diarrhea
Postvagotomy atony
Incomplete vagal transection
11. Early dumping syndrome intake of highly concentrated substances too quickly before they are digested
?concentrated highly osmolar substances travel the shortened distance to the lower intestine quickly
?fluid shift into the small intestine
?release of serotonin, bradykinin-like substances, neurotensin, and enteroglucagon
?cramping, tachycardia, diaphoresis, vomiting, or diarrhea in the early dumping phase (20~30mins)
12. long-acting octreotide for prevention of sym., vasomotor and gastrointestinal
??gastric emptying / ?fasting or interdigestive small bowel motility pattern
?prolongation of intestinal transit of the ingested meal
13. Late dumping syndrome ?absorbing simple sugars in small bowel
?a rapid glucose spike in the blood
?triggering insulin overshooting
?hypoglycemia
?catecholamines release resulting in
diaphoresis, tremulousness,
lightheadedness, tachycardia, and
confusion in late dumping phase (2~3hrs)
14. Ingest frequent small meals and reduce their carbohydrate intake
Use of an antiperistaltic loop of jejunum between the residual gastric pouch and intestine
15. Alkaline reflux gastritis severe epigastric abdominal pain accompanied by bilious vomiting and weight loss
not relieved by food or antacids
vomiting may occur anytime during the day or night
no clear correlation between the volume of bile or its composition and the subsequent development of alkaline reflux gastritis.
No effective medical treatment
16. Nutritional disturbance J CLin Endocrinol Metab 91: 4223-4231,2006
18. Calcium/vit.D deficiency 10%/51% Defective absorption of fat-solubale vit. because of fat malabsorption? steatorrhea
Fat malabsorption is due to the short common channel and delayed mixing of fat with pancreatic enzymes and bile salts as a result of bypassing the duodenum.
bypassing the duodenum and proximal jejunum
further aggravated as fatty acids bind calcium
?markers of bone turnover and/or?bone mass
Metabolic bone disease (osteoporosis/osteomalacia)
calcium carbonate(gastric acid) v.s. calcium citrate
19. Iron-deficiency anemia 52% malabsorption due to bypassing of the duodenum and proximal jejunum, the main sites for iron absorption
intolerance to iron-rich foods, especially red meat
reduced stomach production of hydrochloric acid required to reduce ferric iron to the ferrous state before it can be absorbed.
21. B12 deficiency 64% lower portion of the stomach is removed or partitioned off, chief and parietal cells are lost that secrete hydrochloric acid and intrinsic factor.
pancreatic enzymes as B12 binder proteins are lost as the upper portion of the small intestine
B12 absorption in the distal ileum is calcium-dependent
?B12 prophylactic supplementation with parenteral ,sublingual or intranasal preparations
23. Folate deficiency 38% Primary reason for folate deficiency is decreased folate intake.
Malabsorption may not play a big role,
? because absorption can occur along the entire part of the small intestine with adaptation after surgery
?prevent megaloblastic anemia
24. Protein malnourishment small pouch size ?extremely diminished amount of calorie intake
bulk of digestion occurs in the small intestine/ loss of gastric/pancreatic enzymes? animal proteins more difficult for bypass patients to digest and absorb.
? Muscle catabolism and wasting
25. Gallbladder stone weight reduction with low-calorie diet, incidence of gallstones increases
mechanism not completely understood,
?increased saturation of bile and stasis
?increased gall-bladder secretion of mucin and calcium
?increased presence of prostaglandins and arachidonic acid
Ursodeoxycholic acid administered effective in preventing gallstone formation
26. Thanks !