Download
1 / 31
370 likes | 1.06k Views
Elder Abuse and Neglect. Barbara J. Chromy. What is elder abuse?. an all-inclusive term representing all types of mistreatment or abusive behavior toward older adults (Wolf, 2000, p.7) further defined as acts of commission (intentional behavior) and omission (failure to act)

E N D
Elder Abuse and Neglect Barbara J. Chromy
What is elder abuse? • an all-inclusive term representing all types of mistreatment or abusive behavior toward older adults (Wolf, 2000, p.7) • further defined as acts of commission (intentional behavior) and omission (failure to act) • self-neglect is the most common form of elder abuse and the most difficult to detect and treat (Levine, 2003 and Reynolds Welfel et al., 2000)
Physical Psychological Sexual Material Violation of Rights Medical Abandonment Neglect Self-neglect Types of Abuse
Forms of Abuse Physical - hitting, pushing, slapping, punching, restraining, pinching, force-feeding, physical restraint Psychological - verbal aggression, intimidation, threats, humiliation Sexual - any kind of non-consensual sexual contact
Forms of Abuse (continued) Material - theft of cash or personal property, forced contracts, misuse of income or other financial resources Violationof Rights - deprivation of any inalienable right such as voting, assembly, speech, privacy, personal liberty Medical - withholding medication or overmedicating
Forms of Abuse (continued) Abandonment - desertion of an elderly person for whom one has agreed to care for, “dumping” a cognitively impaired elder at an emergency room with no identification Neglect - failure to provide necessary physical or mental care of an elderly person Self-neglect - behavior that threatens one’s own health or safety
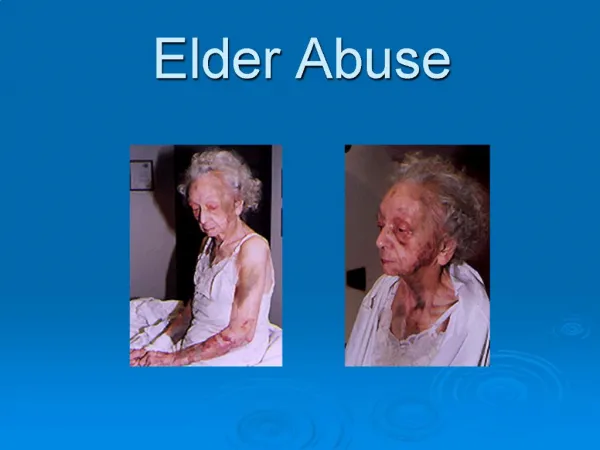
Indications of Abuse Physical - multiple fractures or bruises at various stages of healing, burns, patterned injuries, patchy hair loss, frequent visits to ER, delay in seeking medical treatment for injuries Psychological - withdrawn behavior, wasting or failure to thrive, depression Sexual - genital injury, vaginal or rectal bleeding, bruises, chipped teeth, sexually transmitted disease or infestations
Indications of Abuse (continued) Material - unexplained loss of income, assets, possessions, not eating, missed utility payments Violation of Rights - isolation, failure to attend church services or community events as one did previously Medical - no improvement in condition for which one was prescribed medication, blood tests indicate greater or lower than expected levels of medications, sleepiness, groggy
Indications of Abuse (continued) Abandonment - isolation, not seen outside home, disrepair or unkempt environment, missed medical or other appointments or engagements, wandering, being left somewhere to fend for self Neglect - uncared for appearance, inappropriate clothing, failure to thrive, lack of medical or dental care, isolation Self-neglect – (similar to neglect)
Scope of the Problem • estimates of the occurrence of elder abuse vary widely— due in part to the variability in the definitions used to measure and report abuse • “mistreatment of adults, including abuse, neglect, and exploitation, affects more than 1.8 million older Americans”(Pavlik, Hyman, Festa, Bitondo, and Dyer, 2001, p. 45) • self-neglect accounts for one-third to one-half of all abuse cases(Gray-Vickrey, 2000, 2004; Levine, 2003; Paris, 2003)
Distribution of Abuse • distribution of abuse according to sex was reported by Wolf (2000) to be almost equally divided between males and females • Some studies indicate that females are more often victims of elder abuse (Bratteli2003, Pavlik et al., 2001) • Patterns of abuse are similar among African Americans, Latinos, Caucasians, and Asians (Cavanaugh & Blanchard- Fields cited in Etaugh & Bridges, 2004)
Perpetrators of Abuse • elder abuse can be perpetrated by nearly anyone including paid or volunteer caregivers, medical and long-term care employees, family members, significant others, and in some cases strangers such as a person who befriends an elderly person for the purpose of exploiting them (Reynolds Welfel et al., 2000)
being male under age 60 being related history of mental illness recent decline in mental health abusing alcohol primary caregiver lives with or has access to the adult they abuse change in family roles from being cared for to being the care provider prior history of violence (Bratteli, 2003) Greatest Risk Factors for Causing Abuse in North Dakota
affects of caregiver stress (situational model) dependency of elder on caregiver (exchange theory) mental or emotional disturbance of caregiver (psychopathology) repeated cycle of violence (social learning theory) power imbalance in relationships (feminist theory) marginalization of the elderly within society (political economic theory) Theories Explaining Elder Abuse
Poor health Inability to perform activities of daily living Cognitive impairment Living with others (living alone increases risk for financial and self-abuse) Social isolation Depression, confusion, substance abuse or dependence Mental or physical impairment (stroke, incontinence, Alzheimer’s) Being female Over age 85 Risk Factors for Being Abuses
Risk Factors for Perpetrating Abuse • History of family violence • Disruptive behavior on behalf of the care recipient • Mental illness • Alcohol or drug abuse or dependence • Caregiver dependence
Perpetrating Risk Factors (continued) • Stress • Physical or emotional exhaustion • Low social integration and/or unemployment • Lack of community supports • Insufficient income for basic needs
Protective Measures • Stay sociable and active • Stay involved with neighbors, friends, church or community activities • Get regular medical and dental care • Open and post your own mail • Increase social network as you age • Have friends visit you at home • Have a “best friend” with whom you can confide in • Keep in touch with old friends if you move
Protective Measures (continued) • Keep your possession organized • Tell someone you trust where your important paperwork and bank account information is kept • Have checks direct deposited into your account • Use an answering machine to screen phone calls • Don’t leave cash or valuables visible • Notify the police if you will be away from home for an extended time period
Protective Measures (continued) • Consult with an attorney • Make arrangement for the future such as power of attorney • Get legal advise before making/signing agreements regarding your care or possessions • Be aware of your financial situation
Protective Measures (continued) • Know where to ask for help • Find out about community resources before you need them such as rape and abuse hotlines, senior centers, and adult protective services • mental health service centers • crisis centers • private counselors • clergy • local police
Detection and Treatment Barriers • detection of elder abuse is difficult because denial is an integral feature of abuse, victims may feel too ashamed to disclose maltreatment or believe they are to blame for or deserve the abuse • dependence on an abuser can make a victim reluctant to report for fear of how he/she will survives without the perpetrators help
Detection/Treatment Barriers(continued) • victims may not define their situation as abuse especially in a dysfunctional family environment where violence or mistreatment has been “normalized” (Brown et al., 2004, Levine, 2003) • cognitive, auditory, speech, visual impairments, isolation or restraint may make reporting impossible for the victim of elder abuse
Detection/Treatment Barriers(continued) • ageism can negatively affect detection of elder abuse as it is common to view the elderly as confused or demented, to trivialize elders’ complaints, and to adhere to the perception that elder abuse doesn’t exist • physical injuries may be masked by clothing or by isolating the victim
Detection/Treatment Barriers(continued) • fast paced medical services and heavy caseloads of social service providers may not allow time for adequate assessment • basic lack of information of where to turn for help impedes the intervention and treatment for both perpetrator and victim of abuse
Recommendations • further research using standardized definitions and subtypes of elder abuse would provide a better picture of the scope of the problem • improved reporting guidelines along with increasing the number of agencies and their funding is essential.
Recommendations (continued) • Greater understanding of the causation of elder abuse could lead to the development of effective treatment programs for abusers • defining elder abuse in its own terms rather that modifying guidelines from child abuse legislation would improve the understanding of elder abuse as a phenomenon separate and unique from child abuse
References • Bratteli, M. (2003). Caregiver abuse, neglect and exploitation: The journey through caregiving. North Dakota State University. • Brown, K., Streubert, G., & Burgess, A. (2004). Effectively detect and manage elder abuse. The Nurse Practitioner, 9 (8), 22-33. • Etaugh, C. & Bridges, J. (2004). The psychology of women: A lifespan perspective (2nd Ed.). Boston, MA: Pearson Education, Inc. • Gray-Vickrey, P. (2000). Protecting the older adult: Learn how to assess the visible and invisible indicators and what to do if you recognize abuse in an older patient. Nursing, 30 (7), 34-38.
References (continued) • Gray-Vickrey, P. (2004). Combating elder abuse: Here’s what to look for, what to ask, and how to respond if you suspect that an older patient is a victim. Nursing, 34 (10), 47-51. • Kapp, M., (2004). Family caregivers’ legal concerns. Family Caregiving, (winter) 2003-2004, 49-55. • Lachs, M., & Pillemer, K. (2004). Elder abuse: Seminar. www.thelancet.com, 364 (October), 1263-1272. • Levine. J. (2003). Elder neglect and abuse: A primer for primary care physicians. Geriatrics, 58 (10), 37-45. • Paris, B. (2003). Abuse and neglect: So prevalent yet so elusive (editorial). Geriatrics, 58 (10), 10.
References (continued) • Pavlik, B., Hyman, D., Festa, N., & Bitondo Dyer, C. (2001) Quantifying the problem of abuse and neglect in adults—analysis of a statewide database. Journal of the American Geriatrics Society, 49, 45-48. • Reynolds Welfel, E., Danzinger, P., & Santoro, S. (2000). Mandated reporting of abuse/maltreatment of older adults: A primer for counselors. Journal of Counseling & Development, 78 (summer), 284-292. • Wolf, R., (2001). Introduction: The nature and scope of elder abuse. Generations, Summer, 6-12.
Resources • Aitken, L. & Griffin, G. (1996). Gender issues in elder abuse. Thousand Oaks, CA: Sage Publications, Ltd. • Journal of elder abuse & neglect. Haworth Maltreatment & Trauma Press. • Quinn, M. & Tomita, S. (1997). Elder abuse and neglect: Causes, diagnosis, and intervention strategies (2nd Ed). New York, NY: Springer Publishing Company. • Tatara, T. (1999). Understanding elder abuse in minority populations. Philadelphia, PA: Brunner/Mazel (a member of the Taylor & Francis Group).