Download
1 / 15
150 likes | 365 Views
HIV infected adolescents; an Evolving UK cohort. CJ Foster, EGH Lyall, T Duong, K Doerholt, P Tookey, M Sharland, G Tudor-Williams, V Novelli, K Butler, A Riordan, DM Gibb For. Objective. To describe in adolescents (age 12-19 yrs) in CHIPS : demographic

E N D
HIV infected adolescents; an Evolving UK cohort. CJ Foster, EGH Lyall, T Duong, K Doerholt, P Tookey, M Sharland, G Tudor-Williams, V Novelli, K Butler, A Riordan, DM Gibb For
Objective • To describe in adolescents (age 12-19 yrs) in CHIPS : demographic clinical immunological virological and ART history data
Methods • CHIPS is a collaboration between the National Study of HIV in Pregnancy and Childhood (NSHPC), 19 clinical centres in the UK and Ireland and the MRC Clinical Trials Unit • CHIPS includes all children in follow-up since 1996 in the 19 participating centres • Annual prospective follow up since 2000 with prior retrospective data collection
Demographics of 176 adolescents • 24% of 745 children in CHIPS follow up are adolescents aged between 12-19 years • 99 (56%) female • 151 (86%) vertical transmission, 11 (6%) blood transfusion • 107 (61%) are of Black African origin, 47 (27%) are white • Median age at last follow-up: 14.1 years range (12-19.3)
Case Distribution within UK & Ireland 12 (7%) Scotland 8 (5%) Rest of England 19 (11%) Ireland 137 (78%) London
Mode of presentation (n=176) • 15 (9%) followed from birth • 91 (52%) presented with symptoms 16 CDC category C 35 CDC category B 40 other symptoms • 51 (29%) post diagnosis of family member • 2 (1%) at adoption screening • 1 (0.5%) at antenatal testing • 16 (9%) not known
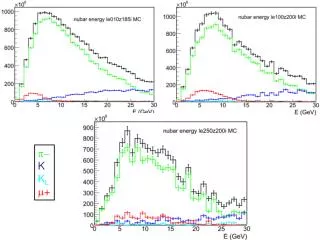
Age at presentation, by calendar year (n=176) 26 children presented aged 12 years old, all since 1997, of whom 21 were born abroad
63 children developed CDC stage Cdiseasesduring follow-up. 4 children have died during adolescent years since 1996
ART history * * 2 received ZDV monotherapy in pregnancy 22/137 children currently alive and previously treated were off treatment at last report
Number of ART drugs ever taken, by whether developed AIDS or not
Transfer to adult care • 20 (11%) transferred to adult care, median age at transfer 17.0 years, range 15.3-18.8 years • 17 in London, 1 Scotland, 2 Ireland • 3 naïve • 10 have developed AIDS Pregnancies 2 reported pregnancies in CHIPS, both were previously naïve and received ZDV monotherapy in pregnancy. • Patient 1: 1999, aged 16 years. CD4%=32%, VL=5562 c/ml. • Patient 2: 2002, aged 15 years. CD4%=37%, VL=3600 c/ml identified at antenatal screening
Conclusions • A quarter of children in the CHIPS cohort have survived to adolescence • More than one quarter of the adolescents have been treated with more than 8 antiretroviral drugs • Almost half of those on treatment have suboptimal virological responses • More than 10% of the adolescents have already transferred to adult services
Acknowledgements We would like to thank the staff, families and infants from the 19 CHIPS centres: Great Ormond Street Hospital for Sick Children, London; St Mary’s Hospital, London; St George’s Hospital, London; Newham General Hospital, London; King’s College Hospital, London; St Thomas’ Hospital, London; Royal Free Hospital, London; Ealing Hospital, London; University Hospital Lewisham, London; Heartlands Hospital, Birmingham; Royal Hospital for Sick Children, Edinburgh; Royal Hospital for Sick Children, Bristol; John Radcliffe Hospital, Oxford; Children’s Hospital, Sheffield; Ninewells Hospital, Dundee; Our Lady’s Hospital, Crumlin, Dublin; Chelsea and Westminster Hospital, London; North Middlesex Hospital, London; University Hospital, Cardiff CHIPS Steering Committee: Karina Butler, Katja Doerholt, David Dunn, Trinh Duong, Di Gibb, Hermione Lyall, Janet Masters, Vas Novelli, Catherine Peckham, Andrew Riordan, Mike Sharland, Pat Tookey, Gillian Wait, Gareth Tudor-Williams National Study of HIV in Pregnancy and Childhood, Institute of Child Health, London: Pat Tookey, Janet Masters, Catherine Peckham Medical Research Council Clinical Trials Unit: Di Gibb, Trinh Duong, Debbie Johnson, David Dunn, Katja Doerholt, Gill Wait, Sarah Walker We also thank the Department of Health, UK for all their support. CHIPS receives also support from Bristol Myers Squibb, Boehringer-Ingelheim, GlaxoSmithKline, Roche and Abbott & Gilead