Download
1 / 25
290 likes | 961 Views
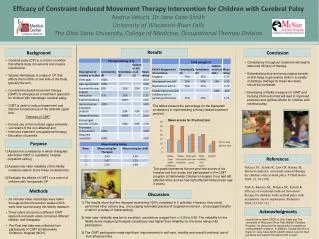
Constraint Induced Therapy: Theory and application in the neurologic population. Valerie Hill Hermann, MS, OTR/L Research Occupational Therapist University of Cincinnati College of Allied Health Sciences Neuromotor Recovery and Rehab Lab valerie.hill@uc.edu. Objectives.

E N D
Constraint Induced Therapy: Theory and application in the neurologic population
Valerie Hill Hermann, MS, OTR/LResearch Occupational TherapistUniversity of CincinnatiCollege of Allied Health SciencesNeuromotor Recovery and Rehab Labvalerie.hill@uc.edu
Objectives • By the end of the seminar the participant will be able to: • Describeconstraint induced therapy, • Identify the main principles of constraint induced therapy, and • Incorporate principles ofconstraint induced therapy into practice
Why is CIMT so popular?CIMT can lead to increased function and changes in the brain…
Functional Magnetic Resonance Imaging Trans-cranial Magnetic Stimulation OT can change the brain
Alternative Pathway - Other areas of the brain assume some function for the damaged area Tissue damaged by stroke - Results in loss of motor function Neuroplasticity: Shown by fMRI
How do Occupational Therapists make neuroplastic changes?!? Via evidence based neurorehabilitation
NeuroRehab Theory:Motor Relearning • Repetitive movement • Active (versus passive!) • Challenging problem-solving tasks • Engaging tasks • Assist only if voluntary movement is inadequate (help the limb be effective in a task) • High dosage • Whole task • Component parts of task
NeuroRehab Theory:Task Oriented Approach • Client Centered • Occupation Based • Person and Environment • Practice and Feedback • Treatment Goals
NeuroRehab Theory:Neurodevelopmental Treatment • Brunnstrom • Bobath • Proprioceptive Neuromuscular Facilitation
NeuroRehab Theory:“Use It or Lose It” • Learned non-use phenomena: • People learn how to NOT use their affected extremities • Results in decreased ability to use whole body • Use dependent cortical reorganization • Brain rewires when forced to use affected extremities
Constraint Induced Therapy • What is CIT/CIMT? • Restraint of less affected arm (aarm) • Forced use of the aarm • Increased practice time • Adaptive task practice • Repetitive task specific practice (15-20 min continuous)
Constraint Induced Therapy • How does it work? • Forces people to engage their aarm • Uses shaping by progressively challenging people, rewarding for success, never blaming for failure • Work on occupation based/ purposeful activities, functional activities/ component parts. • Body and aarm ‘allowed’ to compensate and use synergistic patterning to their advantage
CIT protocol Restraint aarm/hand with a mitt or sling 90% of the time In the clinic 5 days a week 6 hours in clinic 2 weeks mCIT protocol Restraint aarm/hand with a mitt or sling 5 hours per day In the clinic 3 days a week 30 minutes in clinic 10 weeks Constraint Induced Therapy
Constraint Induced Therapy • Other techniques for both protocols: • Patient behavioral contract • Caregiver behavioral contract • Movement monitoring device • Compliance/ homework sheets
EXCITE trial: 1st large RCT of CIMT (Wolf, et al., 2006)
Constraint Induced Therapy • Increases aarm use & function in subacute & chronic patients • TMS- Liepert, 2000 • fMRI- Levy, et al., 2001 • fMRI- Kim, et al., 2004 • Maintained up to one year post • Wolf, et al., 2008 • Repeated practice => brain reorganization => improved motor function
Modified Constraint Induced Therapy • Practice with the aarm 5 hours/day 5 days/week • Patients choose tasks • Reimbursable (reg billing codes) • Less intense than CIMT • What patients are used to
Modified Constraint Induced Therapy Repeated practice => brain reorganization => improved motor function (Page, et al., 2008)
Supplemental treatment ideas to use with CIMT • Saebo • E-stim • Robotics • …
References • Bracciano, A.G. (2008) Physical Agent Modalities: Theory and Application for the Occupational Therapist. (2 Ed). Slack Incorporated. • Kim, Y., Park, J., Ko, M., Jang, S., and Lee, P. (2004) Plastic changes of motor network after constraint induced movement therapy. Yonsei Medical Journal, 454(2):241-246. • Levy, C. E., Nichols, D. S., Schmalbrock, P. M., Keller, P., and Chakeres, D. (2001) Functional MRI evidence of cortical reorganization in upper limb stroke hemiplegia treated with constraint induced therapy. American Journal of Physical Medicine and Rehabilitation, 80(1):4-12. • Liepert, J., Bauder, H., Miltner, W. H., Taub, E., and Weiller, C. (2000) Treatment induced cortical reorganization after stroke in humans. Stroke, 31: 1210. • Page, S.J., Levine, P.G., Leonard, A., Szaflarski, J, P., and Kissela, B. (2008) Modified constraint induced therapy in chronic stroke: results of a single-blinded randomized controlled trial. Physical Therapy, 88: 333-340. • Wolf, S. L., Winstein, C. J., Miller, P., Thompson, P. A., Taub, E., Uswatte, G., Morris, D., Blanton, S., Nicols-Larsen, D., and Clark, P. (2008) Retention of upper limb function in stroke survivors who have received constraint-induced movement therapy: the EXCITE randomized trial. Lancet Neurological, 7:33-40. • Wolf, S.L., Winstein, C.J., Taub, E., Uswatte, G., Morris, D., Giuliani, C., Light, K.E., and Nicholas-Larsen, D. (2006) Effect of constraint induced movement therapy on upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial. Journal of American Medical Association, 296(17); 2141-3.
Questions? Thank you!