Download
1 / 4
0 likes | 2 Views
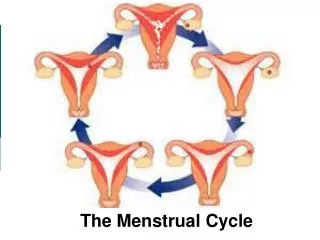
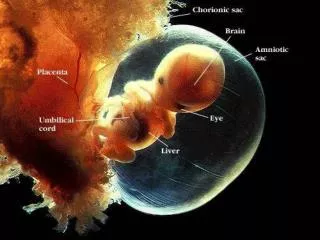
Menstrual Cycle constitutes the cyclical changes, which occur in the ovary and uterus for the purpose of reproduction. The events which occur sequentially in the ovary and uterus prior to ovulation to prepare the right number of follicles to ovulate constitute the follicular phase.

E N D
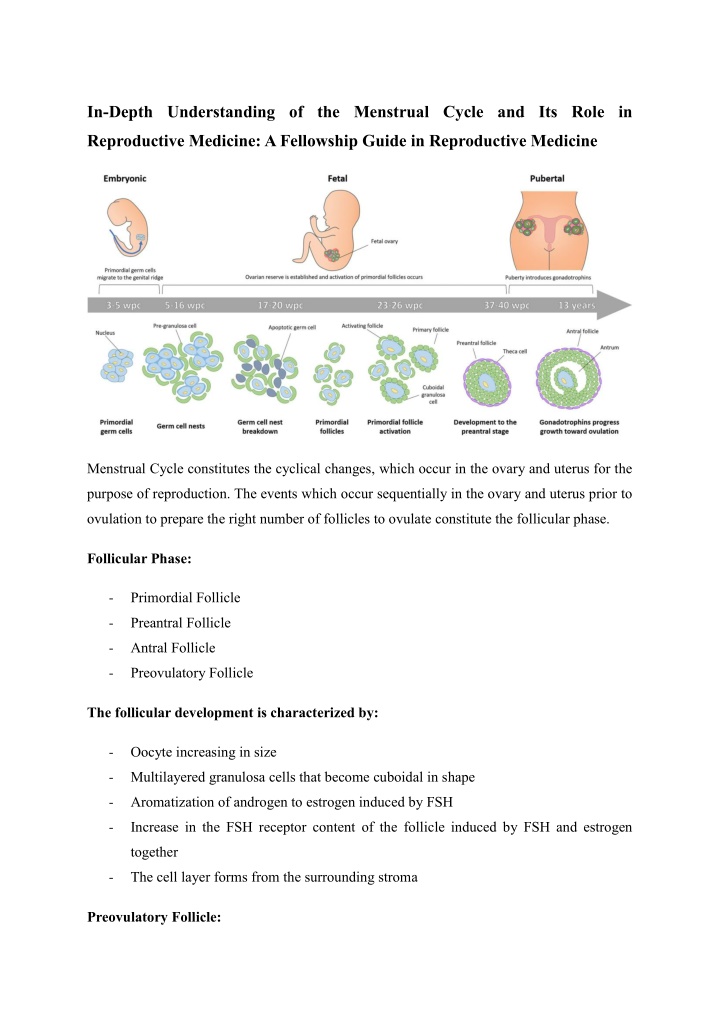
In-Depth Understanding of the Menstrual Cycle and Its Role in Reproductive Medicine: A Fellowship Guide in Reproductive Medicine Menstrual Cycle constitutes the cyclical changes, which occur in the ovary and uterus for the purpose of reproduction. The events which occur sequentially in the ovary and uterus prior to ovulation to prepare the right number of follicles to ovulate constitute the follicular phase. Follicular Phase: -Primordial Follicle -Preantral Follicle -Antral Follicle -Preovulatory Follicle The follicular development is characterized by: -Oocyte increasing in size -Multilayered granulosa cells that become cuboidal in shape -Aromatization of androgen to estrogen induced by FSH -Increase in the FSH receptor content of the follicle induced by FSH and estrogen together -The cell layer forms from the surrounding stroma Preovulatory Follicle:
-Hyperaemic appearance -Enlargement of granulosa cells with acquisition of lipid inclusions -Increased vascularity and assumptions of vacuoles by theca cells -Resumption of oocyte meiosis The increasing oestradiol production in the preovulatory follicle crosses the peripheral threshold to induce positive feedback at the hypothalamic pituitary level and hence the LH surge. -Estradiol concertation must be > 200 pg/mL -Sustained for 50 hrs Timing of the ovulation induction includes: -10-12 hours post the peak in LH Concentration -24-36 hours post the peak in estradiol levels The key events that occur during ovulation include: -Meiosis resumption in Oocyte -Granulosa cells luteinization -Prostaglandins and progesterone syntheses that are required for dissolution of the follicular wall and release of oocyte -Ensure adequate LH receptors for a normal luteal phase For the optimal luteal phase, the following are required: -Satisfactory development of follicles in the preovulatory phase -Continuous tonic LH support in the post ovulatory luteal phase The Luteal-Follicular Transition -Fall in estradiol, progesterone levels -Fall in inhibin levels -Increase frequency of GnRH release from hypothalamus Endometrial changes during the menstrual cycle: -Endometrial epithelial stem cells in the bottom of the endometrial glands
-Stromal stem cells in the basalis layer -The narrow tubular glands initially lined by columnar epithelium become pseudostratified and mitosis becomes prominent -The dense stromal component is converted into a loose syncytium like tissue as a result of stromal edema -The spiral vessels extent up to the basement membrane of the epithelium and forms a loose capillary network. -Decrease in mytosis and DNA synthesis -Decrease estrogen receptor expression -Increased enzyme activity The complex hormonal and physiological interactions of the menstrual cycle are essential to the field of reproductive medicine, which is a key area of focus for the Fellowship in Reproductive Medicine at Medline Academics. Grasping the sequential alterations in the ovary and uterus, including those during the follicular phase, the dynamics of preovulatory follicles, ovulation, and the luteal phase, is vital for managing and treating fertility issues. The process of follicular development, influenced by FSH and estradiol, readies the oocyte for ovulation, with crucial indicators like estradiol levels and LH spikes steering clinical practices such as ovulation induction. Additionally, the luteal phase and the transition between luteal and follicular phases emphasize the necessity of sufficient hormonal support for successful implantation and pregnancy. Concurrently, the changes in the endometrium, driven by cellular restructuring and vascular adjustments, highlight the uterine receptiveness essential for embryo implantation. This thorough comprehension provides fellows with the skills needed to oversee
ovulation induction, luteal phase support, and endometrial preparation, all of which are vital elements of assisted reproductive technologies (ART) and infertility treatment strategies. In India, the Fellowship in IVF seeks to train reproductive specialists through the hybrid form of learning, and it includes a structured approach which is a combination of online learning and clinical practice. The fellows are trained in the fundamental subjects which ART’s triumph depends upon, such as ovulation induction, luteal phase support and endometrial preparation. These Fellowship in Reproductive Medicine in India are further enhanced through simulation training and clinical provision and allow participants to practice embryo transfer and follicular monitoring using ultrasound in a controlled setting. This bridges the gap between what’s learnt and the practical realities of treating patients with complicated infertility challenges. Through these fellowships, India continues to establish itself as a hub for excellence in reproductive healthcare education. As we conclude, the Fellowship in Reproductive Medicine in India provides healthcare professionals with the essential knowledge, skills, and confidence necessary to thrive in the domain of reproductive healthcare. By combining innovative theoretical frameworks, practical clinical experience, and sophisticated simulation training, these programs equip participants to tackle the intricate challenges associated with infertility treatment and assisted reproduction. This holistic methodology not only improves clinical proficiency but also plays a significant role in advancing the future of reproductive medicine both in India and internationally.