Download
1 / 116
1.18k likes | 2.07k Views
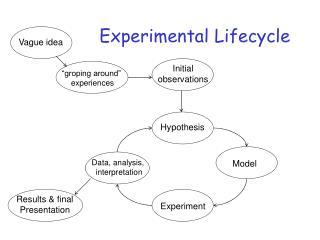
Lifecycle Nutrition. Developmental Nutrition FCSN 345. Dr. Virginia Bennett Office 134 PE Office hours: T & Th 1:00 e-mail: bennettv@cwu.edu. Measures of a Successful Outcome of Pregnancy. Healthy Baby Healthy Mother Baby Survives the First Year of Life. Healthy Baby.

E N D
Developmental NutritionFCSN 345 • Dr. Virginia Bennett • Office 134 PE • Office hours: T & Th 1:00 • e-mail: bennettv@cwu.edu
Measures of a Successful Outcome of Pregnancy • Healthy Baby • Healthy Mother • Baby Survives the First Year of Life
Healthy Baby • Still Birth Ratio or Fetal Death Ratio • Early in Pregnancy: difficult to have reliable numbers of death rate • Why? • Later in Pregnancy: numbers are more reliable after 20 wks gestation • About 6.4 stillbirths per 1000 live births
Healthy Mother: Maternal Mortality • Static since 1982 at 7 to 8 mothers die per 100,000 births. About 1 death per day in the US • Big racial difference: • White 5.0 • Black 20.8 • Others 18.2 • Why?
Infant Mortality • Infancy: First Year of Life • <28 days - neonatal • >28 days < 1 year - postneonatal • 2006: Infant Mortality Rate in US • 6.43 per 1000 live births • Ranked 42nd world-wide • 1950 29.2 but we were ranked 6th world-wide • Why?
terminology • Infant: first year of life • Neonatal: under 28 days of life • Early Neonatal: under 7 days of life • Post neonatal: 28 days – 11 months • Fetal mortality: fetal deaths over 20 weeks gestation • Late Fetal mortality: deaths over 28 weeks gestation
Cause of Infant Problems • Neonatal Problems: first 28 days after birth • What might be the reasons for problems here? • 4.7 in 2002 • Post neonatal Problems: 28 days to one year • What might be the reasons for problems here? • 2.3 in 2002
In US • Most infant deaths happen in neonatal period • Perinatal mortality: adds fetal deaths plus early neonatal deaths
Better Infant Mortality Rates • Japan: 3.24 • Singapore: 2.29 • Sweden: 2.76 • Hong Kong 2.95 • Cuba 6.22 • CIA - The World Factbook -- Rank Order - Infant mortality rate
Risk of Infant Mortality: Factors • If infant mortality rate was similar to Singapore’s we would save over 18,900 infant deaths per year • Low Birth Weight largest single factor • less than 5.5 pounds (2500 grams) • LBW risk factors: • K maternal pre-pregnancy ht & wt and pregnancy weight gain • age socioeconomic poverty • number of pregnancies race
Classification of Low Birth Weight • Premature • < 37 weeks • Intrauterine Growth Retardation or Small for Gestational Age • ³37 weeks • wasted - thin, ¯wt, normal length • stunted - ¯ wt ¯lgth ¯head circum
How to improve Infant Mortality Rate? • Housing • Sanitation • Diet • Health care
Nutrition Influences on Fetal Growth • Deficiency in Calories • Too few Calories to allow adequate reproduction of cells and decreased development • Deficiency of Nutrients • Too little of some specific nutrient • e.g.: folic acid • spina bifida
Winick: Growth Happens in Two Ways • Increased number of cells • Increased size of cells • Critical times of increased number of cells • 1. Increased number hyperplasia • 2. Number and size + hypertrophy • 3. Size Hypertrophy
Critical Periods • If an embryo or fetus doesn’t receive the nutrition necessary to help with development, the fetus will suffer • Fertilization of the ovum(zygote) happens • implantation of the ovum in the uterine wall happens in the first two weeks • Critical period: cigarette smoke, malnutrition can keep development from occurring
Types of Fetal Growth Failure • Intrinsic: some internal factor • chromosome abnormalities • drug affecting cells • Extrinsic: some external factor • poor intake of nutrients • poor blood supply
Is the fetus a perfect parasite? • What does this mean? • Fetus takes what it needs regardless of mother’s intake • Probably isn’t true. • It takes what it needs until it disrupts mother’s ability to survive • From a species survival standpoint: mother needs to survive
Events of Pregnancy • Time Event • 0-2 weeks egg fertilized and implanted • 3-8 weeks Embryo: at end of 8 weeks is 1 inch and has central nervous system, GI tract, limb, buds, etc. • 8-40 weeks Fetal period: growth and development
Role of the Placenta • Nutrient and waste product exchange • Hormone production • Estrogen: helps develop the infrastructure of pregnancy • Progesterone: • Relaxes smooth muscle • Relaxes the uterus • Relaxes the digestive system: slower movement
Placenta Roles • Transport Mechanisms: • Passive Diffusion: • Oxygen -Carbon dioxide • Fatty acids -Steroids • Nucleosides -Electrolytes • Fat-soluble vitamins
Placenta is Selectively Permeable • Not all molecules can cross the placenta • Vitamin D can • Parathyroid Hormone (PTH) can’t • Allows for bone remodeling
Placental Transport • Facilitated Diffusion: • Most monosaccharides • Active Transport: • Amino acids --some cations (Ca, Iron) • Iodine --Phosphate • Water-soluble vitamins (at high concentrations Vitamin C can pass via diffusion) • Solvent Drag: electrolytes
Nutrient Needs to Support Pregnancy • Energy: • No increase in Cal for first trimester • Why?: 1. Very small embryo; 2. Increased absorption of most nutrients and Cal due to decreased motility of GI tract due to hormones of pregnancy • 300 Cal increase during 2nd and 3rd trimester
Nutrient Needs During Pregnancy • Protein: • Determine pre-pregnancy needs based on RDA: 0.8 grams protein/kg. This is generally around 45 to 50 grams Protein per day. • Add 15 grams to this for pregnancy • Generally around 60 to 65 grams/day is sufficient
Methylated Molecule Molecule SAM SAH Homocysteine Methionine Methyl-H4 Folate H4 Folate B12 serine glycine Methylene-H4 Folate purine Purine precursor
Nutrients of Special Interest • Folate: related to neural tube defects and spina bifida • Reduced absorption during pregnancy because of interaction with estrogen • Produces folate deficient women • Interferes with proper formation of spinal column: affects 400,000 births per year • Folate supplements during pregnancy required
Nutrients of Special Interest • Iron: Blood volume increases by 50% during pregnancy • Body conserves Iron during pregnancy • No menstruation • 3 time increase in absorption • But still doesn’t keep up with production of red blood cells • Hemoglobin concentration falls: normal above 13 g/dl. In pregnancy may fall below 12 g/dl • RDA up from 15 to 30 mg/day
Special Supplemental Food Program for Women, Infants, and Children • To battle against problems during pregnancy and infancy, WIC was developed to provide supplemental food to low socioeconomic and at risk women and infants. • Nutrition education also provided • Recent study: for each $1 spent, $4 save down the road; • Avg costs: Normal Birth Weight= $1,700; Premie or low birth weight = $77,000
Information on WIC • http://www.fns.usda.gov/wic/ • In 2005 we had about 8 million receiving WIC assistance in the US; This cost about $1.4 Billion • In 2005 we had about 160,000 receiving WIC assistance in Washington; This cost about $28 Million dollars
Body Mass Index • Kg/ meters 2 • 175#/2.2 #/kg = 79.5 kg • 72 “ X .0254 meters/inch = 1.83 meters • 1.83 meters 2 = 3.35 79.5 / 3.35 = 23.7
Weight Gain During Pregnancy • Based on Pre-pregnancy BMI • Underweight (BMI<19.8) : 28-40 # • Normal weight(BMI 19.8-26) : 25 to 35 # • Overweight(BMI 26-29): 15 to 25 # • Obese(BMI over 29): 13 # minimum • Other Modifiers: Small stature(<62 in) : low end of range; black: high end of range
Wt Gain for multifetal pregnancies • Twins: 35-45 lbs. Underwt at the upper end of range; overwt at the lower end • 4-6 lb first trimester; 1.5 lb/wk after • 450 Cal per day above prepregnancy amount • Triplets: 50 lbs with 1.5 lb/wk throughout pregnancy • Cal intake should reflect enough intake to meet wt gain goals
Average weight of multifetal pregnancies • Singletons: 7.7 lbs(3440 grams) • Mean gestational age: 39-40 wks • 6% lbw • Twins: 5.4 lbs(2400 grams) • 37 weeks; 54 % lbw • Triplets: 4.0 lbs(1800 grams) • 33-34 wks; 90% lbw
Rate of Weight Gain • First Trimester: 2 to 4 pounds • Second and Third Trimester: 1 pound per week • 3 pounds + (26 weeks x 1 # per week) = 29#
Components of Weight Gain • Infant 7.5 # amniotic fluid 2 # • Placenta 1.5 # mother’s stores 7 # • Blood 4 # • Fluid 4 # • uterus 2 # • Breasts 2 # • TOTAL 30 #
Fetal Alcohol Syndrome • Physical and Mental Abnormalities attributed to alcohol consumption during pregnancy • low nasal bridge small head • short nose circumference • short eyelid opening delayed • thin upper lip development • underdeveloped filtrum
Source of FAS Information • http://www.nofas.org/ • http://capwiz.com/nofas/issues/alert/?alertid=6804721&type=CO • Advocacy Extra credit assignment: write a letter to your members of congress
FAS Screening • In 1996, FAS Facial Photographic Screening/Diagnostic software (Astley & Clarren, 1996;2001;Astley et al., 2001;Astley & Kinzel, 2002). The software is used to measure the magnitude of expression of the three facial features of FAS (small eyes, a smooth philtrum and a thin upper lip).
FAS Screening • FAS is characterized by growth deficiency, a unique cluster of facial features, cognitive/behavioral problems and prenatal alcohol exposure. The facial appearance is the only feature that is unique to FAS, thus it serves as an ideal feature to use for screening. The screening tool performed with 99.9% accuracy.
Alcohol Effects on Pregnancy • About 1/5 of women continue to during pregnancy • The first few weeks are critical; many women don’t know they are pregnant • Birth defects have occurred in women who consume as little as two drinks per day • No alcohol is the best if planning pregnancy • Fetal Alcohol Effects: internal damage
Other Dietary Concerns during Pregnancy • Caffeine: • Animal models: massive doses are teratogenic • Smaller doses not as definitive • mixed results in epidemiological studies • generally if caffeine is consumed, it should be moderately
Sugar Substitutes • Saccharin: A carcinogen? Limit during pregnancy • Doses relationship: high intake = greater risk • Aspartame (Nutrasweet): • PKU mothers should avoid • If not PKU, moderate intake probably ok but need to increase Cal (2nd and 3rd trimesters) and Calcium
Maternal Problems of Pregnancy • Gestational Diabetes: Glucose Intolerance • Hormones of pregnancy make mother’s body resistant to insulin;Human Placental Lactogen (HPL); Human Growth Hormone(HGH) • Often shows up at 25 weeks of pregnancy • Needs to be treated to control growth of the fetus • Macrosomia: large baby and delivery complications