Download
1 / 40
410 likes | 600 Views
Mental Health Diagnostic and Procedural Coding. Objective. To improve diagnostic and procedural coding for mental health screening, assessment, referral, and intervention. How Do Y ou D ocument M ental H ealth S ervices ?. Who documents mental health services?

E N D
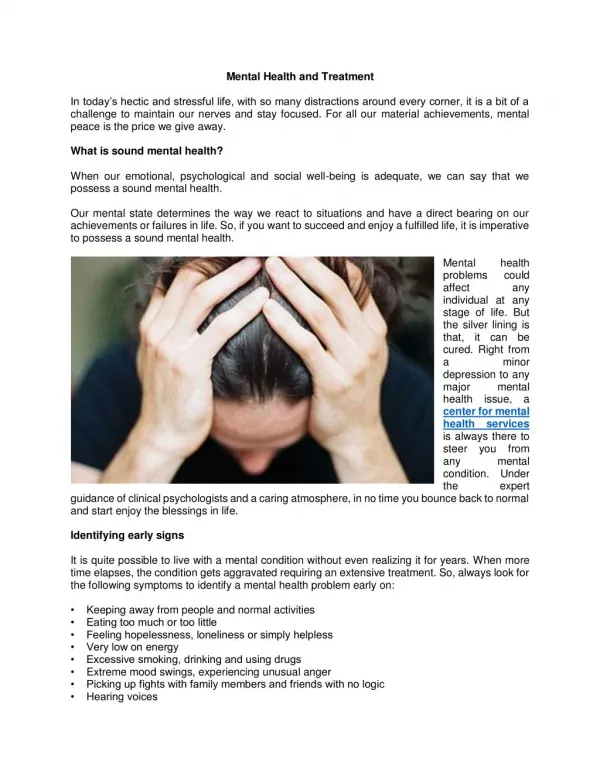
Mental Health Diagnostic and Procedural Coding
Objective To improve diagnostic and procedural coding for mental health screening, assessment, referral, and intervention
How Do You Document Mental Health Services? • Who documents mental health services? • Where are mental health services documented? (mental health chart, medical record, both charts, log sheet, database, encounter form) • How do mental health providers and primary care providers share information about mental health services?
What We’ll Cover… • Why code? • General Coding Principles • Mental Health Diagnostic Codes • Mental Health Procedural Codes • Reimbursement • Who can bill? • Fraud and Abuse • Work plan suggestions
“We can’t bill for mental health services, so why code?” You should still document in order to: • Justify your position • Assess mental health problems of school population • Track treatment • Track compliance • Assist in measuring outcomes • Demonstrate a need for mental health reimbursement
Why Code Correctly? • Reimbursement depends on services described by CPT codes--coding is the basis for reimbursement • Diagnosis codes support medical necessity for services delivered • Understanding coding assumptions and guidelines helps providers to optimize reimbursement • Providers must establish integrity in the health care system • Document necessity services • Illustrate complexity of services
General Coding Principles • The purpose of codes is to document services provided • Documented services are likely to be paid • Services not documented “never happened” • Never “upcode” for the purpose of getting more money • Most likely, you are undercoding
General Coding Principles (cont) • Two Part Coding Process • CPT – “What you do” • ICD – “Why you do it” • Diagnosis codes (ICD) must support procedure codes (CPT) You must always have both!
General Coding Principles (cont) • Primary Steps for Coding an Encounter: • Provider chooses procedure code (CPT) from encounter form or superbill • Provider notes diagnosis, which is matched to a diagnosis code (ICD)
Documentation Where to document codes? • Encounter Form • Database BOTH (if separate): • mental health chart AND • medical record
Coding Systems ICD-9-CM(International Classification of Diseases, Ninth Revision, Clinical Modification) • Used by health care professionals to classify patient illnesses, injuries, and risk factors *ICD-10 coming out in 2012 DSM-IV-TR(Diagnostic and Statistical Manual – Fourth Edition – Text Revised) • Used by mental health clinicians to make a psychiatric diagnosis *DSV-V coming out in 2013
Anxiety Disorders 300.01 Panic Disorder Without Agoraphobia 300.21 Panic Disorder With Agoraphobia 300.22 Agoraphobia Without History of Panic Disorder 300.29 Specific Phobia Specify type: Animal Type/Natural Environment Type/Blood- Injection-Injury Type/Situational Type/Other Type 300.23 Social Phobia Specify if Generalized 300.3 Obsessive-Compulsive Disorder Specify if With Poor insight 309.81 Posttraumatic Stress Disorder Specify if Acute/Chronic Specify if With Delayed Onset 308.3 Acute Stress Disorder 300.02 Generalized Anxiety Disorder 300.00 Anxiety Disorder NOS
Depressive Disorders • 296.xx Major Depressive Disorder • .2x Single Episode • .3x Recurrent • 300.4 Dysthymic Disorder Specify if Early Onset/Late Onset Specify With Atypical Features • 311 Depressive Disorder NOS
Disruptive Behavior Disorders • 314.xx Attention-Deficit/Hyperactivity Disorder • .01 Combined Type • .00 Predominantly Inattentive Type • .01 Predominantly Hyperactive-Impulsive Type • 314.9 Attention-Deficit/Hyperactivity Disorder NOS • 312.xx Conduct Disorder • .81 Childhood-Onset Type • .82 Adolescent-Onset Type • .89 Unspecified Onset • 313.81 Oppositional Defiant Disorder • 312.9 Disruptive Behavior Disorder NOS
Substance Abuse/Dependence • 303.90 Alcohol Dependence/305.00 Alcohol Abuse • 304.00 Amphetamine Dependence/305.70 Amphetamine Abuse • 304.30 Cannabis Dependence/305.20 Cannabis Abuse • 304.20 Cocaine Dependence/305.60 Cocaine Abuse • 304.50 Hallucinogen Dependence/305.30 Hallucinogen Abuse • 304.60 Inhalant Dependence/305.90 Inhalant Abuse • 305.1 Nicotine Dependence • 304.00 Opioid Dependence/305.50 Opioid Abuse • 304.60 Phencyclidine Dependence/305.90 Phencyclidine Abuse • 304.10 Sedative, Hypnotic, or Anxiolytic Dependence/305.40 Sedative, Hypnotic, or Anxiolytic Abuse • 304.80 Polysubstance Dependence • 304.90 Other (or Unknown) Substance Dependence • 305.90 Other (or Unknown) Substance Abuse The following specifiers apply to Substance Dependence as noted: With Psychological Dependence/Without Psychological Dependence Early Full Remission/Early Partial Remission/Sustained Full Remission/Sustained Partial Remission In a Contained Environment On Agonist Therapy
Documentation of Diagnostic Codes • Report the full ICD-9-CM code for the diagnosis shown to be chiefly responsible for the outpatient services. • Providers should report the diagnosis to their highest degree of certainty.
Coding Systems • CPT (Current Procedural Terminology) - codes that predominantly describe services & procedures. • They provide a common billing language that providers and payers can use for payment purposes
Evaluation & Management (E&M) Codes • 99201 – 99215 New and Established Patient Office Visits • 99241 - 99245 Consultations • 99361 - 99362 Case Management Services, Team Conferences • 99371 - 99373 Case Management Services, Telephonic
Mental Health Procedure Codes • 90801 - 90802 Psychiatric Diagnostic or Evaluative Interview Procedures • 90804 - 90829 Psychotherapy • 90804 - 90815 Office or Other Outpatient Facility • 90810 - 90815 Interactive Psychotherapy • 90816 - 90829 Inpatient Hospital, Partial Hospital or Residential Care Facility • 90845 - 90857 Other Psychotherapy • 90862 - 90889 Other Psychiatric Services or Procedures
Psychiatric Therapeutic Procedures • CPT Codes 90804 – 90889 • Psychotherapy is the treatment for mental illness and behavioral disturbances in which the clinician establishes a professional contract with the patient and, through definitive therapeutic communication, attempts to alleviate the emotional disturbances, reverse or change maladaptive patterns of behavior, and encourage personality growth and development.
E&M Codes and MH Codes • The Evaluation and Management services should not be reported separately, when reporting codes: 90805, 90807, 90809, 90811, 90813, 90815, 90817, 90819, 90822, 90824, 90827, 90829
Reimbursement • Who can bill? • Fraud and Abuse
Who Can Bill? • What are the rules governing who can bill for mental health diagnosis/treatment in your state?
Who Can Bill? • Who can bill for behavioral health services? • Most states accept physicians, Clinician Psychologists (CP), Licensed Clinical Social Workers (LCSW) • However, each State has its own rules and many will pay for other professionals
Coverage Issues • A provider should know what services are covered. • Services must be documented and medically necessary in order for payment to be made. • Do you, as a provider, know if all services provided are covered? • Are you documenting properly, and what about this “medically necessary” bit?
How Much Are You Paid? Reimbursement • Reductions in reimbursement rates by provider type • Physician - not discounted • Clinical Psychologist - discounted • LCSW - further discounted • Other - discounted if covered
Reimbursement Issues • E&M codes are limited to physicians, Pas, NPs, nurses • Same is true for 90805, 90807, 90809 codes • An E&M (992XX) and a therapy (908XX) cannot be billed on the same date of service to most Medicaid programs
Documentation and Coding:Fraud and Abuse • Services MUST be medically necessary (determined by payers based on a review of services billed) • Music, game, instrument, pet interaction therapies, sing-alongs, arts and crafts, and other similar activities should not be billed as group or individual activities. • Services performed by a non-licensed provider particularly as “incident to” using the PIN of the licensed provider
Elements of “Incident To” • An integral part of the physician’s professional service • Commonly rendered without charge or generally not itemized separately in the physician’s bill • Of a type that are commonly furnished in physician’s office or clinic • Furnished under the physician’s direct personal supervision
Action Step:Review Program Services • Define the Behavioral/Mental Health Services your students are receiving • Determine if there are additional Behavioral/Mental Health Services you want to provide
Action Step:Review and Modify Encounter Form • Does encounter form include both diagnostic and procedural codes that would be used for behavioral health when delivered by primary care providers? Mental health providers? • Do procedural codes represent all services provided (including those not billed for)? • Do diagnostic codes represent all diagnostic categories (including those not billed for)?
Action Step:Review and Modify Documentation Procedures • Are diagnostic and procedure codes documented for in each progress note? • Are codes for each encounter documented in both the SBHC medical record and mental health chart (if separate)? • Are codes entered into database regardless of reimbursement?
Action Step:Understand State Program and Provider Coverage Issues • Research State Program Information • www.cms.gov (Medicare Regulations) • Search by state by Department of Health or Department of Mental Health to find state specific information • Contact State Medicaid Assistance Program and determine specific Behavioral Health Service requirements • Invite Medicaid Representatives to your facility or visit them to present Behavioral Health Program and clearly understand the requirements
Questions to Answer • What criteria must programs (SBHC) meet in order to provide behavioral health services? • What providers are eligible to provide behavioral health services? • What are your state’s credentialing and licensing requirements for providers of behavioral health services? • What credentialing and licensing requirements are necessary for billing in your state? • What are the guidelines for billing services as “incident to?”
Action Step:Determine Reimbursement Estimates • Obtain reimbursement rates by provider type for state and other programs • Understand billing rules by payer, e.g. billing E&M visit same day as Behavioral Health visit, number of visits limits, auth/pre-authorizations, etc. • Assure you have a complete understanding of program parameters re: Individual Therapy, Case Management, Special Behavioral Health Services, etc.