Download
1 / 26
280 likes | 946 Views
Crohn’s Disease. Public Health 256 Molecular and Genetic Epidemiology Fall 2000. Natural History. Inflammatory Bowel Disease (IBD) Crohn’s Disease (CD) Ulcerative Colitis (UC) Prevalence Occurrence Symptoms. Inflammatory Bowel Disease. Ulcerative Colitis

E N D
Crohn’s Disease Public Health 256 Molecular and Genetic Epidemiology Fall 2000
Natural History • Inflammatory Bowel Disease (IBD) • Crohn’s Disease (CD) • Ulcerative Colitis (UC) • Prevalence • Occurrence • Symptoms
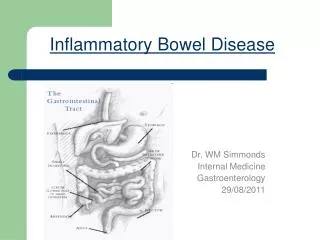
Inflammatory Bowel Disease • Ulcerative Colitis • Inflammation of the lining of the large intestine or colon • Crohn’s Disease • Inflammation extends deeper into the lining of the intestine and usually occurs in the first part of the large intestine (cecum) and the ileum
Anatomy of IBD Location of the ileocecal region; cecum, ileum and ileocecal valve
Symptoms of IBD • Loss of appetite • Bloody diarrhea • Abdominal pain • Fever • Growth failure • Anemia
IBD Occurrence • Most often diagnosed between the ages of 15 and 40 (30% between the ages of 10-19) • About 2% in children under the age of 10 • A lesser peak between the ages of 50 and 80
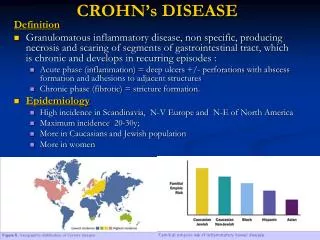
CD Incidence Rates • CD 1-10 per 100,000/yr in the U.S. • Incidence has been increasing slowly world-wide • Highest rates in Scandinavian Countries and Scotland followed by England and North America • Uncommon in developing countries
Crohn’s Disease Hypothesis Targan and Murphy, 1995 LUMEN Lumenal bacterial antigens/products 1 Mucosal immune system Th1 v. Th2 response Level/duration of cytokine response Resistance to Normal downregulators Tissue Injury/ineffective repair 2 4 5 3 Th2 T Severity of disease Th1 GENETIC SUSCEPTIBILITY • 2 3 4 • Number of genes
Heritability of CD • Heritability is greater for CD than UC • Strong evidence from twin studies, familial risk data, and segregation analysis • Complex genetic trait as inheritance does not follow any simple Mendelian models. • Recessive Model with reduced penetrance and polygenic multifactorial inheritance
Genetics of CDFrom the OMIM: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=OMIM • IBD has been linked to 16p12-q13 (IBD1), 12p13 (IBD2) and 6p (IBD3). • Hugot et al, 1996 identified the susceptibility locus to be centered around D16S409 and D16S419 • Cavanaugh, et al 1998; Australian families 1.7cM region between D16S409 and D16S753
HLA and CD • HLA class II DR or DQ alleles are associated with CD, and the DPB1*0401 allele was shown to be associated with CD as compared to UC. This association is not due to linkage disequilibrium with the previously defined DR/DQ regions, but represents an independent risk factor.
Unknown Etiology of CD • Infectious agent(s)? • Vaccines? • Diet (refined sugar and starch consumption)? • Fast food? • Perinatal infections?
Molecular Genetics Leads to Cure • “Knowing the genes and related immunologic markers of a given patient would define subgroups and direct therapy to most effectively combat the array of abnormalities by separate, or sequential therapies. A goal for the future is to define the most central abnormalities, for example, Th1 imbalance, and direct therapy to this point, bringing the inflammation into remission, and to follow with antigen(s)-specific therapy.” (Targan and Murphy, 1995)
Evaluating whether Crohn’s Disease might have a genetic component . . . A) geographical variation
Evaluating whether Crohn’s Disease might have a genetic component . . . B) descriptive epidemiology: ethnic variations Ashkenazi Jews outside Israel > inside Israel Northern Europe>North American >Japan>developing countries
Evaluating whether Crohn’s Disease might have a genetic component . . . C) family history ~ 10% to 25% of probands have positive family history D) familial aggregation relative risk for CD in siblings = 36.5 highest risk among first-degree relatives Age adjusted risk estimate for CD: 3.9% of first degree relatives E) family clustering risk of CD in sibs / risk of CD in general population = 15 ~ 35
How familial studies have elucidated information on Crohn’s:
How twin studies have elucidated information on Crohn’s: Twin studies: Sweden - twin registry - 44 pairs with IBD; heritability of liability ( r ) proportion of variance of normally distributed liability which is genetic; range 0-1 r reflects the genetic contribution to the disease manifestation monozygotic twins: r = 1.0 (0.8 - 1.0) dizygotic twins: r=0.47 (0.20-0.73)
How familial studies have elucidated information on Crohn’s: Concordance between family members > random assortment age of onset within 10 years (68%) type of disease (88%) Differentiating aspects to familial disease as compared to sporadic disease
How epidemiology and its study designs have elucidated some of the genetic aspects to Crohn’s disease ... A genetic heterogeneity model would hold that Crohn’s disease is not a single disease but is rather several, perhaps etiologically and phenotypically distinct, diseases presenting a similar clinical picture. Each of the individual component disorders conceivably could be inherited in a Mendelian, multigenic mode, perhaps with environmental influences affecting the expression of disease (Bayless, 1996)
Complex Segregation Analyses of a Family Study with 265 Patients With Crohn Disease and 5,387 Relatives Kuster, W., et al. Am J. Medical Genetics (32):105-8, 1989 Suggests that a recessive gene with low penetrance affects susceptibility to Crohn disease.
Segregation Analysis • Issues: • mode of inheritance • penetrance • genetic heterogeneity
Public health implications and applications of understanding the genetics behind Crohn’s disease: • risk -- genetic anticipation • treatment • etiology - genetics vs. environment • research studies