Download
1 / 29
380 likes | 1.35k Views
Neuromuscular Disease. Stacy Rudnicki, MD Department of Neurology. Disorders of the Motor Unit. Motor neuron disease Peripheral nerve disorders Neuromuscular junction disease Muscle disease. Motor Neuron Disease.

E N D
Neuromuscular Disease Stacy Rudnicki, MD Department of Neurology
Disorders of the Motor Unit • Motor neuron disease • Peripheral nerve disorders • Neuromuscular junction disease • Muscle disease
Motor Neuron Disease • Diseases that can involve Betz cells of the motor cortex, the lower CN motor nuclei, the CST, and/or the anterior horn cells • Amyotrophic Lateral Sclerosis (ALS) • Progressive bulbar palsy • Progressive muscular atrophy, spinal muscular atrophy • Primary lateral sclerosis
ALS • Loss of motor neurons in the cortex, brainstem and spinal cord • Mix of upper motor neuron and lower motor neuron findings • Weakness, atrophy, fasciculations • Slurred speech, difficulty swallowing, shortness of breath • Can start in any extremity or the bulbar musculature • Relentlessly progressive
ALS • 50 % dead in 3 years, 80% dead in 5 years, 5-10% live more than 10 years • Death usually from respiratory failure • Etiology still only theoretical • Excess glutamate • Oxidative stress • Free radicals • Mitochondrial dysfunction
Peripheral Nerve Disorders • Mononeuropathy • Pattern of weakness and sensory loss conforms to the distribution of a single nerve • Carpal tunnel syndrome • Peroneal palsy at the fibular head • Mononeuritis multiplex • Multiple nerves affected in a random pattern • Acute onset, frequently painful • Diabetes mellitus, vasculitis • Polyneuropathy (peripheral neuropathy) • Distal, symmetric
Polyneuropathies • Can affect different types of fibers • Autonomic • Motor • Sensory • Large well myelinated • Small poorly myelinated or unmyelinated
Symptoms of a Polyneuropathy • Sensory symptoms • Start in feet, move proximally • Hand sxs appear when LE sxs up to knees • Positive • Pins and needles • Tingling • Burning • Negative • Numbness • Deadness • “Like I’m walking with thick socks on”
Polyneuropathy Symptoms, cont • Motor • Weakness first in feet • Tripping • Turn ankles • Progress to weakness in hands • Trouble opening jars • Trouble turning key in lock
Polyneuropathy: Signs • Distal sensory loss • Large fiber • Small fiber • Distal weakness and atrophy • Decreased or absent reflexes • Ankle jerks lost first
Classification of Polyneuropathies • By types of fibers involved • Pure sensory • Sensory motor • Pure motor • Autonomic • By pathology • Demyelinating • Axonal • Mixed • By tempo • Acute • Subacute • Chronic
Acute Polyneuropathies • Guillain Barre Syndrome • Porphyria • Neuropathy, psychiatric disorder, unexplained GI complaints • Toxins • Glue sniffing (n-hexane) • Arsenic
Guillain Barre Syndrome • Most common cause of rapidly progressive weakness • Demyelinating neuropathy • Ascending weakness which may include cranial neuropathies • Exam reveals symmetric weakness with areflexia and large fiber sensory loss • Bowel and bladder usually preserved
Guillain Barre Syndrome, cont • Respiratory failure can be precipitous • Other causes of morbidity and mortality • Autonomic instability • DVT • Infection • Immune mediated, may be post infectious • Treatment • Plasma exchange • Intravenous immunoglobulin
Subacute Polyneuropathies • Vasculitis • Can be isolated to peripheral nerves or part of a more systemic process • Paraneoplastic • May be presenting symptom of the cancer • Chronic inflammatory demyelinating polyneuropathy • With or without a gammopathy • Toxins • Drug
Chronic Polyneuropathies • Metabolic • Diabetes mellitus • Chronic renal failure • Chronic liver failure • Thyroid disease • Nutritional • B12 deficiency • Infections • HIV • Leprosy • Inherited
Evaluation of a Polyneuropathy • Lab work • Nerve conduction study/electromyography • Distinguishes between axonal and demyelinating • Helps ascertain severity • Nerve biopsy • Frequently non-diagnostic • Can establish the dx in certain disorders, such as vasculitis and amyloidosis
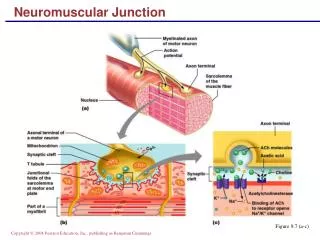
NMJ • Pre-synaptic • Lambert Eaton myasthenic syndrome • Botulism • Post-synaptic • Myasthenia Gravis
Myasthenia Gravis • Antibody that alters the acetylcholine receptor • Binding • Blocking • Modulating • Antibody detected in • 50% of pts with pure ocular MG • 90-95% of pts with generalized MG
Clinical Manifestation of MG • Sxs worsen with exercise, end of day (Fatigue) • Ocular • Droopy eyelids (ptosis) • Double vision (diplopia) • Extremity weakness • Arms > legs • Bulbar • Dysarthria • Dysphagia • Respiratory • Shortness of breath
Approach to treating MG • Remove any exacerbating factors • Infections, medication, endocrine disease • Acetylcholinesterase inhibitors • Plasma exchange/ intravenous immunoglobulin • Thymectomy • Immunosuppressants • Prednisone • Imuran (azathioprin)
Clinical Manifestations of Myopathies • Proximal muscle weakness • Waddling gait • Difficulty climbing stairs • Trouble lifting arms over head • Cramps with the metabolic myopathies • Myalgias with the inflammatory myopathies • Swallowing and breathing difficulties, when present, are usually late
Classification of Muscle Disease • Dystrophies • Duchenne’s Muscular Dystrophy • Myotonic Dystrophy • Congenital Myopathies • Glycogenoses • Mitochondrial • Acquired Myopathies • Polymyositis • Dermatomyositis • Inclusion body myositis • Drug related
Duchenne’s Muscular Dystrophy • X-linked recessive • Absence of dystrophin protein • Slow to reach motor milestones, sxs by age 5 • All walk, may never run • End up in wheelchair by age 10-12 • Steroids may delay time until wheelchair bound • Muscles replaced by fat may appear hypertrophic • Frequently mildly mentally retarded • Life expectancy < 20 years with death related to respiratory failure or cardiomyopathy
Polymyositis • Presents with proximal muscle weakness in 92% • Myalgias in 25% • Associated symptoms may include fever, weight loss • Slightly increased risk of cancer • Bladder, lung, lymphoma • Biopsy of muscle confirms diagnosis • Treatment with immunosuppression • Prednisone • Methotrexate
Evaluation of the Patient with Suspected Muscle Disease • Lab • Muscle enzymes (CPK, aldolase) • Erythrocyte sedimentation rate (ESR or sed rate) if suspect inflammatory disease • Genetic test • Duchenne’s • Myotonic dystrophy • EMG/NCS • Muscle biopsy • May provide a definitive diagnosis
Extremity CN Reflexes Sensation Weakness ALS Random yes Increased Normal Polyneuro- Distal> rare Decreased Lost distally > pathy Proximal distally proximally LEMS LE > UE rare Decreased or Normal Prox>distal absent MG UE>LE yes Normal or dec Normal +/-prox>distal Myopathy Prox>distal occ Normal or dec Normal