Download
1 / 39
400 likes | 736 Views
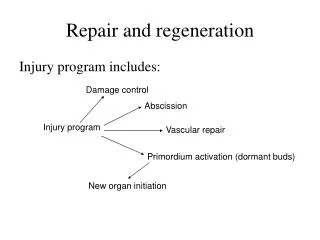
Preclinical Animal Models of Cartilage Repair and Regeneration. Matthew J. Allen, Vet. M.B., Ph.D. Associate Professor, Orthopedic Surgery SUNY Upstate Medical University, Syracuse, New York. Overview. Why use animal models to study cartilage repair?

E N D
Preclinical Animal Models of Cartilage Repair and Regeneration Matthew J. Allen, Vet. M.B., Ph.D. Associate Professor, Orthopedic Surgery SUNY Upstate Medical University, Syracuse, New York
Overview • Why use animal models to study cartilage repair? • What is the question that is being asked • Mechanistic vs. proof of concept vs. dose finding vs. safety and efficacy • Identification of the most appropriate animal model • Each of the commonly used models has advantages and disadvantages • Rational selection of outcome measures and time points • Practical recommendations • Initial screening • Pivotal testing for safety and efficacy • Limitations of current animal models
Why Use Animal Models? • Many key issues relating to chondrocyte differentiation and function can be studied in vitro • In-vitro tests can also be used to characterize the interactions between cells and matrices • Animal tests are however critical to explore • cell growth and differentiation within an articular environment • local and systemic safety • stability of cell function, marker expression and mechanical properties of the neocartilage • long-term effects of tissue remodeling within and around the repair site
Purpose of the Study • Mechanistic study of basic biological processes • Preliminary dose-finding study • physical intervention (e.g. drilling) • cellular therapy • gene or growth factor therapies • “A versus B” study (comparison with predicate treatment) • prove that it is at least as good as an existing therapy • Pivotal safety and efficacy study for new treatment • what constitutes efficacy? • statistical versus biological significance • accuracy, sensitivity and relevance of safety studies
Available Models • Rodent (mouse, rat) • Rabbit • Nonhuman primate • Pig • Small ruminants (sheep, goat) • Horse
Key Issues in Repair Models • Age and its effect on skeletal turnover • Bilateral versus unilateral surgery (IACUC issue) • One- or two-stage surgery (IACUC issue) • Nature of the implant • Autogenous or allogeneic cells • Composition of the scaffold • Size (area, depth) and location of the lesion • Partial or full thickness, critical or non-critical size • Weight-bearing versus non-weight bearing location • Appropriate surgical controls • Same site, perhaps from the contralateral limb
Which is the Best Model? • “Best” should refer to relevance to humans but it is also impacted by practical considerations such as • Cost (short studies in small animals are least expensive!) • Availability of facilities, equipment and skilled personnel • Comparative anatomy and joint function • Surgical access to the articular surface • Larger joints provide more cartilage • Larger joints may also permit arthroscopic procedures • Rehabilitation protocols • Outcome measures • In-life and post-mortem • One model may not be ideal for every stage of testing
Goat Pig * Human* Sheep * Dog Rabbit Rat Mouse Skeletal Anatomy * Bellemans, 1999
Outcome Measures • Clinical function • force plate, pain scores, ROM etc. • Visual assessment • 2nd look arthroscopy ± biopsy versus necropsy • Imaging • radiography and MRI (requires general anesthesia) • Histology • standardization of sampling and scoring schemes • Mechanical testing • Marker analysis • biochemical analysis of synovial fluid • molecular analysis of tissue samples
MRI and Cartilage • Development of standardized MRI protocols for cartilage would be helpful in animal studies • repeated measures in the same animal • Newer techniques such as dGEMRIC appear to be very useful in humans but practical application in large animal models will be problematic • High field strength magnet required • Delayed analysis may necessitate unacceptably long anesthesia times
Histological Analysis • Two scoring schemes are widely used • O’Driscoll • Pineda • Tissue sampling protocols should be developed • These should focus on both the repair site and the “healthy” tissue around the repair • Identification of the margins and the center of the original lesion is critical • Contemporary (not historical) controls should be included whenever possible • A combination of tinctorial and immunohistochemical staining provides maximum information
Mechanical Testing • Compression testing • Confined or unconfined • Indentation testing • Potentially useful in vivo as a means of assessing the repair • As with all analyses, relevant controls are critical • Ultimately, though, the properties of a “good” repair have not yet been fully defined • assumption is that repair tissue should behave like hyaline cartilage
Scaling from Animals to Humans • Inter-species variations in many biological processes can be related to changes in body size • What about cartilage? Kleiber, 1947
Cartilage Thickness Based on the following sources: Changoor et al., 2004 (horse); Shepherd and Seedhom, 1997 (human); Jackson et al., 2001 (goat); Lane et al., 2004 (goat); Gelse et al., 2003 (rat); Oakley et al., 2004 (sheep); Hunziker and Rosenberg 1996 (rabbit, minipig)
Chondrocyte Morphometry Hunziker and Quinn, 2003
Scaling Volumes and Areas • Cartilage lesions represent a volume of tissue loss • For a standardized lesion, healing potential should depend on the area (?) • Given their inherent biological differences, animal models should only really be expected to provide relative (rather than absolute) information on healing rates for new therapies
Scaling Defects Thickness Density Extent of the Defect Human Rabbit Goat H R G H R G 0% 95% 85% Marrow contact from Hunziker, 1999
Trochlea groove Femoral condyle Location of Defects
Autologous Chondrocyte Implantation • Modeling ACI generally requires two procedures • initial tissue harvest • implantation of cells with/without scaffold • In inbred animals, an alternative would be to evaluate syngeneic cells • One-step procedures are being evaluated in animal models (Bertone et al., 2005) • cartilage broken up and seeded onto scaffold materials
Autologous Chondrocytes • ACI has been performed in • Rabbits (Brittberg et al., 1996) • Sheep (Russlies et al., 2005) • Dogs (Breinan et al., 1997) • Goats (Vasara et al., 2004) • Horses (Litzke et al., 2004) • Failures have been associated with • Displacement of the periosteal patch • Intrinsic problems with the animal models?
Surgical Technique -- ACI www.carticel.com
Autologous Chondrocytes • Graft locations appears to have an impact, as in humans • No clear guidance exists for lesion size, cell density etc. • Studies should evaluate a range of cell doses since this is, in effect, what happens in clinical ACI • Future work will focus on enhancing the proliferation, survival and/or function of transplanted cells • In this context, ex-vivo gene therapy appears to offer tremendous potential
Bone Marrow Stromal Cells • BMSCs have the potential to differentiate into chondrocytes in vitro and in vivo • Limited number of studies have been performed in animal models • Rabbits (Diduch et al., 2000) • Appealing concept since the cells can be expanded and manipulated ex vivo, prior to being re-implanted • Potential concerns remain, including the potential for de-differentiation • In animal models, BMSC collection may necessitate general anesthesia
Allogeneic Cells • Genetically modified cells have been evaluated extensively in horses • BMP-7, IGF-1, TGF- • Application of allogeneic or xenogeneic cells is appealing • eliminates the need for two surgeries • permits the use of cells from young donors • Potential draw-backs are • immunogenicity • disease transmission • Animal models must explore immune response as well as potential local/systemic toxicity of growth factors
Osteochondral Grafts • Studies in goats, sheep, dogs and horses all support the potential of autograft and allograft osteochondral transfer to repair lesions • Concerns remain about • Autograft donor site morbidity • Long-term survival of implanted chondrocytes • Snap frozen less good than cryopreserved • In humans, viability decreases after 14 days of storage (Williams et al., 2003) • Immune response to allograft OCT poorly understood • Differences in the mechanical properties of cartilage from different sites • Irregularities in the surface contour at the recipient site
OCT in the Goat *Lane et al., 1999
The Limitation of Animal Models “Although the repair of articular cartilage defects has been studied in many species including rabbits, goats, and sheep, there is no consensus on the most appropriate animal model….” “…none of these species replicate the anatomical, cellular, and biomechanical properties of the human knee. Therefore, we selected the most closely related species, a nonhuman primate (NHP), that may exhibit a healing response most similar to that of humans….” Gill et al., AJSM, 2005
Current Recommendations • Preliminary, short-term proof of concept can be performed in rabbits • Definitive tests of efficacy in small lesions can be performed in the goat • Feasible at most institutions • Already established as the standard model • Confirmatory studies of efficacy in large lesions can only really be performed in the horse
Issues for Consideration • What is the appropriate scaling factor for cell-based therapies? • Are there inherent differences between chondrocytes from different species • differences are known to exist between young and aged cells • response to growth factors can be variable • What is the ideal rehabilitation protocol? Is this practical? • best for the animal vs. most relevant to humans • Are clinical outcomes in animals predictive of those in humans? • How long do we need to follow animals?
Immune Responses • Disruption of the subchondral bone permits vascular access and immune recognition • Fresh osteochondral grafts are highly immunogenic • Freezing reduces immunogenicity, probably by reducing the transfer or donor leucocytes • Studies in dogs have documented both cell-based and humoral responses against MHC determinants • Since immune responses are known to diminish long-term function, attention must be paid to evaluating these responses in vivo
Summary • No single animal model is ideal for all stages of testing (this is often true) • A rational approach would be to screen strategies in small animals and then confirm in large animals • Emphasis should be on • safety • confirmation that the strategy is at least as effective as the current benchmark • Ultimately, controlled clinical trials are needed to document long-term efficacy