Download
1 / 36
400 likes | 1.35k Views
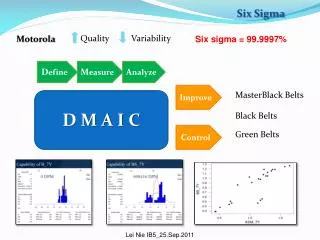
Fall Prevention Utilizing Six Sigma Methodologies to Improve Patient Outcomes. Presented by : Virtua’s Fall Prevention Team. What is Six Sigma?… . Methodology for achieving goals and objectives Quantitative technique for problem solving Comprehensive improvement process.

E N D
Fall Prevention Utilizing Six Sigma Methodologies to Improve Patient Outcomes Presented by: Virtua’s Fall Prevention Team
What is Six Sigma?… • Methodology for achieving goals and objectives • Quantitative technique for problem solving • Comprehensive improvement process Tools For Driving Sustainable Change
DMAIC Define Define Deliverables • Develop Team Charter • Identify Project Critical to Quality (CTQ’s) • Define Process Map
DMAIC Team Charter • Identify Project Team and Role assignments • Describe Project • Align with Strategic Imperatives • Delineate Timelines • Define Scope of Project • Identify Business Units • Analyze Constraints • Assess Project Benefits • Identify Project Goal • Evaluate Possible Barriers to Success
DMAIC Opportunity Statement
DMAIC Voice of the Customer (VOC)! VOC was captured to understand the problem from the customers perspective
DMAIC High Level Process Map
DMAIC Stakeholder Analysis Who Strongly Opposed Opposed Neutral Supportive Strongly Supportive Not all stakeholders are supportive of the initiative…now what?
How it comes together ... DMAIC At the end of define, we knew: • Why this project is important. • What business goals the project must achieve to be considered successful. • Who the key stakeholders are on the project. • What limitations have been placed on this project. • What key process is involved. • What are the customers’ needs and expectations.
DMAIC Measure Measure Deliverables • Define performance metrics • Determine customer specifications and defects • Identify potential variables • Develop data collection plan • Establish process capability
DMAIC What is the right “Y” to measure? VOC Customer Need Prioritized Project Y • Decrease patient falls • Effective and efficient bed alarms • Call bells answered in a timely manner • Standardized falls prevention education process • All hospital staff proactive with awareness of falls prevention • High risk patients identified accurately and placed on proper precautions CTQ: Inpatient falls are below or equal to 3/1000 pt days # of inpatient falls Target: < or equal to 3/1000 pt days CTQ: 100% accuracy in falls assessment on admission
DMAIC Acute Care Detailed Process Map Patient falls during hospital stay
DMAIC Initial Cause and Effect Diagram
DMAIC Data Collection • Developed data collection plan • Performed “gauge R and R” • Developed data collection guidelines • Determined acceptable sample size needed for chart review • Performed extensive chart review of all fall patients
DMAIC How are we doing?
DMAIC How it comes together ... At the end of measure, the team had/knew: • A list of potential variables • The critical input, process and output measures • The measurement system was accurate • What patterns were exhibited in the data • What the current process capability was
DMAIC Analyze Analyze Deliverables • Identify variation sources • Establish performance objectives
DMAIC Cause and Effect Diagram C : Constant = something that doesn’t change N : Noise = something that adds variability to our Y yet can’t be helped X : X = a factor that drives our Y
DMAIC Impact/Effort Grid • Nurses’ interpretation of the Morse Scale • Fall score day of fall • Medication within 6 hours of fall • Patient age • Location in room • Mental status the day of the fall • Orientation on the day of the fall High/Low High/High 1 2 4 3 Low/Low Low/High 7 5 6 Impact Effort
What did we learn from Analyze? Information collected from chart reviews • Inconsistencies in documentation • Fall score lowered day before fall: 38% • Neuro section of the nursing flow sheet discrepancies: 18% • Patient’s orientation on the day of fall was not reflected in the scoring of mental status on the Morse scale • No existing documentation on effectiveness of interventions • Confusion with the use and interpretation of the Morse Scale as an assessment tool • Inconsistent application of the intervention protocol resulted in patients falling multiple times during their hospital stay • Lack of documentation supporting changes made to the fall score *Based on 154 charts reviewed
What did we learn from Analyze? • Change of shift 88% did not fall during shift change • Location of fall 82% fell near the bed • Day of the week No statistical significance • Time of the day No statistical significance • LOS No statistical significance Based on 154 charts reviewed
Survey results • 77% of Nurses surveyed felt the Morse scale is not an effective assessment tool (Sample: 100) • 42% of staff surveyed felt that *standard interventions are not effective (Sample:100) • 36% of staff surveyed felt bed alarms are effective, but the response time is an issue (Sample:100) • 60% are not aware of the amount of falls occurring on their units (Sample:124) • 74% are aware of the falls safe program (Sample:124) *two side rails, magenta (safety) bands
DMAIC How it comes together ... By the end of the Analyze Phase, the team was able to show which causes they would focus on in the Improvement Phase by describing: • Which potential causes they identified • Which causes they decided to investigate and why • What data they collected to verify those causes • How the data was interpreted
DMAIC Improve Improve Deliverables A. Screen Potential Causes *List of Vital Few “X’s” B. Discover Variable Relationships *Propose Solutions C. Establish Operating Tolerances *Pilot Solution
DMAIC Root Cause Analysis
DMAIC Pre-pilot Activities The team followed a specific algorithm to complete task in preparation of the pilot.
DMAIC Findings from Observations • No consistency in interventions used • Staff opinions varied on which interventions were in use • No standard process for rounding • Many employees were not aware of unit fall rates • Most employees had no knowledge of unit action plans • Nurses expressed difficulty interpreting Morse Scale • Patients identified at high risk were not easily found when reviewing pts charts • Fall precautions were not often followed on all patients identified at risk for falls • Staff could not easily identify patients at risk for falls
DMAIC Standard Improvement Strategies for Pilot • Educate staff on the process, importance of rounding, expectations and accountability • Educate nurses on the appropriate use of the Morse Scale • Consistency in initiating the “4 P’s” during hourly patient rounds (rounding with a purpose) • Post unit results in appropriate (visible) area as a constant reminder to staff: “how are we doing with patient falls” to increase staff awareness • Consistency in the use of standard interventions (magenta bands, two bed rails, personal items within reach, bed alarms (where applicable), falling star, chair alarms (where applicable) • Discuss patients at high risk during morning huddles to increase awareness * 4 P’s = Pain, Position, Potty (Toileting) and Personal Items
DMAIC Pilot Plan Purpose: • Implement improvement strategies while monitoring performance and effectiveness of process and interventions to reduce preventable falls due to inconsistent practice Where/Who: • 2 nursing units identified with a high volume of patient falls (4N- Marlton, 4NE Memorial) • 4 Members of the fall prevention team would work with staff to implement improvement strategies, making adjustments as needed • Staff would be surveyed on the perception of the current practice Timelines: • 3/15/10-5/17/10 Debrief Sessions: • Bi-weekly starting: 3/31/10 (Wednesday’s)
Pilot Plan- continued Procedures: • New procedures documented in SOP format • Other materials needed and instructions were developed Staffing: • Utilizing existing staffing • Fall prevention core team would be available for consultation purposes Stakeholders: • Extensive information about pilot was communicated to all (appropriate) key stakeholders. • All involved in the pilot were updated and educated accordingly. Measurements: • See attached data collection plan to monitor key indicators. • Methods/tools developed to document what works, what doesn’t and who would respond to unanticipated problems.
Result! Metrics Page for Discrete Data DMAIC 4NE-Memorial 4N-Marlton
DMAIC FMEA FMEA was completed and recommended actions included: • Implementing rounding with a purpose • Standardizing system for accountability and follow-through • Documenting factual narrative description of the event • Utilizing post falls assessment form • Discussing falls patients during interdisciplinary rounds • Including Pharmacy in interdisciplinary rounds once a week
Fall Prevention Improve Prioritizing the Variables to achieve Six Sigma! Rounding with a Purpose: Audit tool and SOP’s, Badge Buddies, 4P’s, PCT rounding expectations (with and without clock). Falls will be standing item on unit based council agenda. Post Falls Assessment: Requesting all elements to be available in Peminic. Model under development. Interdisciplinary Rounds: Daily goal sheet and shift report, encouraged to ask “what level of risk is patient?” instead of “Is patient at risk?”. Mandatory standard use of falling star intervention. Staff Awareness: Daily and weekly monitoring tool. Falls banner to increase staff awareness. Fall Education: Redesigned falls (online) education. Fall simulation developed for clinical orientation. Education developed for clinical and non-clinical support service departments DMAIC
DMAIC Next Steps for Control • Inform organizational leaders of the changes made to the process • Develop tools needed to sustain improvement (Control plan, SOP’s, Virtual Tool Box, Informational share point sites, etc.) • Communicate changes made to the process to key stakeholders Virtua wide • Educate key stakeholders on the process Virtua wide • Roll out and implementation of improvement strategies Virtua Wide
Questions? Reducing variation to achieve 6 sigma one defect at a time!