Download
1 / 1
40 likes | 409 Views
Chronic Thromboembolic Pulmonary Hypertension in an Asian Female Lee Licheng, MD 1 , Fukuyama Osamu, MD 2 1,2 Department of Medicine, University of Hawaii John A. Burns School of Medicine, Honolulu, HI, USA. . INTRODUCTION. ELECTROCARDIOGRAM. VENTILATION/PERFUSION SCAN. DISCUSSION .

E N D
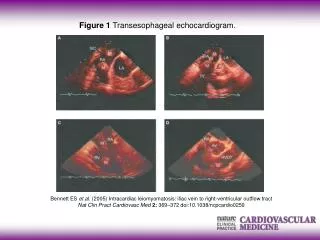
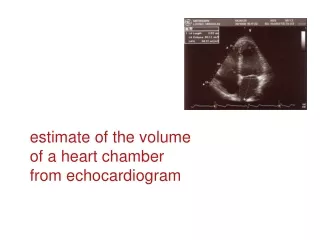
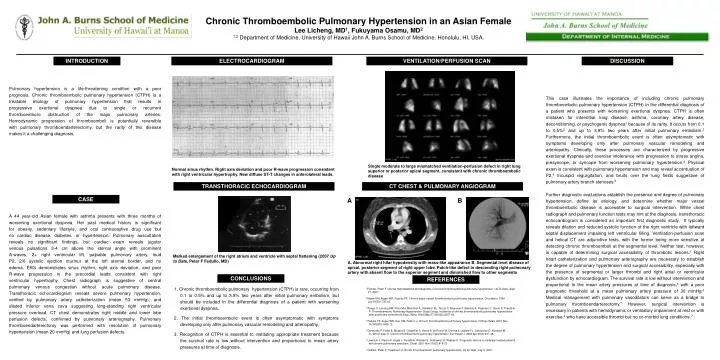
Chronic Thromboembolic Pulmonary Hypertension in an Asian Female Lee Licheng, MD1, Fukuyama Osamu, MD2 1,2 Department of Medicine, University of Hawaii John A. Burns School of Medicine, Honolulu, HI, USA. INTRODUCTION ELECTROCARDIOGRAM VENTILATION/PERFUSION SCAN DISCUSSION Pulmonary hypertension is a life-threatening condition with a poorprognosis. Chronic thromboembolic pulmonary hypertension (CTPH) is atreatable etiology of pulmonary hypertension that results inprogressive exertional dyspnea due to single or recurrentthromboembolic obstruction of the major pulmonary arteries.Hemodynamic progression of thromboemboli is potentially reversiblewith pulmonary thromboendarterectomy, but the rarity of this diseasemakes it a challenging diagnosis. This case illustrates the importance of including chronic pulmonary thromboembolic pulmonary hypertension (CTPH) in the differential diagnosis of a patient who presents with worsening exertional dyspnea. CTPH is often mistaken for interstitial lung disease, asthma, coronary artery disease, deconditioning, or psychogenic dyspnea1 because of its rarity. It occurs from 0.1 to 0.5%2 and up to 3.8% two years after initial pulmonary embolism.3 Furthermore, the initial thromboembolic event is often asymptomatic with symptoms developing only after pulmonary vascular remodeling and arteriopathy. Clinically, these processes are characterized by progressive exertional dyspnea and exercise intolerance with progression to stress angina, presyncope, or syncope from worsening pulmonary hypertension.4 Physical exam is consistent with pulmonary hypertension and may reveal accentuation of P2,4 tricuspid regurgitation, and bruits over the lung fields suggestive of pulmonary artery branch stenoses.5 Further diagnostic evaluations establish the presence and degree of pulmonary hypertension, define its etiology, and determine whether major vessel thromboembolic disease is accessible to surgical intervention. While chest radiograph and pulmonary function tests may hint at the diagnosis, transthoracic echocardiogram is considered an important first diagnostic study. It typically reveals dilation and reduced systolic function of the right ventricle with leftward septal displacement impairing left ventricular filling. Ventilation-perfusion scan and helical CT are adjunctive tests, with the former being more sensitive at detecting chronic thromboemboli at the segmental level. Neither test, however, is capable of determining surgical accessibility of thrombotic lesions.1 Right heart catheterization and pulmonary arteriography are necessary to establish the degree of pulmonary hypertension and surgical accessibility, especially with the presence of segmental or larger thrombi and right atrial or ventricular dysfunction by echocardiogram. The survival rate is low without intervention and proportional to the mean artery pressures at time of diagnosis,4 with a poor prognostic threshold at a mean pulmonary artery pressure of 30 mmHg.6 Medical management with pulmonary vasodilators can serve as a bridge to pulmonary thromboendarterectomy.7 However, surgical intervention is necessary in patients with hemodynamic or ventilatory impairment at rest or with exercise,4 who have accessible thrombi but no co-morbid lung conditions.7 Single moderate to large mismatched ventilation-perfusion defect in right lung superior or posterior apical segment, consistent with chronic thromboembolic disease Normal sinus rhythm. Right axis deviation and poor R-wave progression consistent with right ventricular hypertrophy. New diffuse ST-T changes in anterolateral leads. TRANSTHORACIC ECHOCARDIOGRAM CT CHEST & PULMONARY ANGIOGRAM CASE A B A 44 year-old Asian female with asthma presents with three months ofworsening exertional dyspnea. Her past medical history is significantfor obesity, sedentary lifestyle, and oral contraceptive drug use butno cardiac disease, diabetes, or hypertension. Pulmonary auscultationreveals no significant findings, but cardiac exam reveals jugularvenous pulsations 3-4 cm above the sternal angle with prominentA-waves, 2+ right ventricular lift, palpable pulmonary artery, loudP2, 2/6 systolic ejection murmur at the left sternal border, and noedema. EKG demonstrates sinus rhythm, right axis deviation, and poorR-wave progression in the precordial leads consistent with rightventricular hypertrophy. Chest radiograph is suggestive of centralpulmonary venous congestion without acute pulmonary disease.Transthoracic echocardiogram reveals severe pulmonary hypertension,verified by pulmonary artery catheterization (mean 53 mmHg), anddilated inferior vena cava suggesting long-standing right ventricularpressure overload. CT chest demonstrates right middle and lower lobeperfusion defects, confirmed by pulmonary arteriography. Pulmonarythromboendarterectomy was performed with resolution of pulmonaryhypertension (mean 20 mmHg) and lung perfusion defects. Marked enlargement of the right atrium and ventricle with septal flattening (2007 Up to Date, Peter F Fedullo, MD) A. Abnormal right hilar hypodensity with mass-like appearance B. Segmental level disease of apical, posterior segment of right upper lobe. Patch-like defect in descending right pulmonary artery with absent flow to the superior segment and diminished flow to other segments CONCLUSIONS REFERENCES 1. Chronic thromboembolic pulmonary hypertension (CTPH) is rare, occurring from 0.1 to 0.5% and up to 3.8% two years after initial pulmonary embolism, but should be included in the differential diagnosis of a patient with worsening exertional dyspnea. 2. The initial thromboembolic event is often asymptomatic with symptoms developing only after pulmonary vascular remodeling and arteriopathy. 3. Recognition of CTPH is essential to instituting appropriate treatment because the survival rate is low without intervention and proportional to mean artery pressures at time of diagnosis. 1 Fedullo, Peter F. Clinical manifestations and diagnosis of chronic thromboembolic pulmonary hypertension. Up To Date, Sept 21, 2007. 2 Moser KM, Auger WR, Fedullo PF. Chronic major-vessel thromboembolic pulmonary hypertension. Circulation. 1990 Jun;81(6):1735-43. 3 Pengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, Albanese P, Biasiolo A, Pegoraro C, Iliceto S, Prandoni P; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism.N Engl J Med. 2004 May 27;350(22):2257-64. 4 Fedullo PF, Auger WR, Kerr KM, Rubin LJ. Chronic thromboembolic pulmonary hypertension. N Engl J Med. 2001 Nov 15;345(20):1465-72. 5 Dartevelle P, Fadel E, Mussot S, Chapelier A, Hervé P, de Perrot M, Cerrina J, Ladurie FL, Lehouerou D, Humbert M, O, Simonneau G. Chronic thromboembolic pulmonary hypertension. Eur Respir J. 2004 Apr;23(4):637-48. 6 Lewczuk J, Piszko P, Jagas J, Porada A, Wójciak S, Sobkowicz B, Wrabec K. Prognostic factors in medically treated patients with chronic pulmonary embolism. Chest. 2001 Mar;119(3):818-23. 7 Fedullo, Peter F. Treatment of chronic thromboembolic pulmonary hypertension. Up To Date, July 5, 2007.