Download
1 / 56
690 likes | 6.63k Views
Neuroanatomy of UMN and LMN Motor Speech Disorders. ASHA Presentation November 19, 2009 Susan T. Jackson. Disorders Causing UMN and LMN Speech Disorders. Stroke (UMN, LMN) ALS (UMN and LMN) CP (UMN, LMN) Tumor (UMN, LMN) Trauma (UMN, LMN) MS (UMN, LMN) Wilson’s disease (UMN)

E N D
Neuroanatomy of UMN and LMN Motor Speech Disorders ASHA Presentation November 19, 2009 Susan T. Jackson
Disorders Causing UMN and LMN Speech Disorders • Stroke (UMN, LMN) • ALS (UMN and LMN) • CP (UMN, LMN) • Tumor (UMN, LMN) • Trauma (UMN, LMN) • MS (UMN, LMN) • Wilson’s disease (UMN) http://www.ninds.nih.gov/disorders/wilsons/wilsons.htm • Myasthenia Gravis (LMN) http://www.ninds.nih.gov/disorders/myasthenia_gravis/myasthenia_gravis.htm • Bell’s palsy (LMN) • Guillain-Barré Syndrome (LMN) http://www.ninds.nih.gov/disorders/gbs/gbs.htm
Dysarthrias that Result from UMN and/or LMN Damage • Spastic dysarthria • Stroke, CP, tumor, trauma, encephalitis • Flaccid dysarthria • Stroke, CP, tumor, trauma, Bell’s palsy, Myasthenia Gravis, Guillain-Barré Syndrome • Mixed spastic-flaccid dysarthria • Stroke, trauma, ALS • Mixed spastic-ataxic-hypokinetic • Wilson’s disease • Variable (spastic-ataxic-flaccid) • MS
Nerve Fibers • Three types: commissural, association, projection • These fibers are white matter, and they are bundles of axons • Commissural fibers – connect the two cerebral hemispheres. The corpus callosum is the largest, and is the main conveyor of inter-hemispheric info. • Association fibers – connect areas of the brain within the same hemisphere. Long association fibers are known as fasciculi. Fasciculi are large bundles of axons. There are three major fasciculi, but we’ll mention one – the arcuate fasciculus. It connects Broca’s area with Wernicke’s area, and lies one inch below the cortex. • Projection fibers - connect areas of the cortex with lower levels of the nervous system
Projection Fibers • Efferent projection fibers are motor (they carry info from the cortex) • Afferent fibers are sensory (they carry info to the cortex) • Efferent motor fibers originate in the pre-central gyrus and in the area of the frontal lobe anterior to the pre-central gyrus. They innervate cranial nerve nuclei in the brainstem or cells in the spinal cord. • Afferent sensory projection fibers originate in sensory receptor cells and their destination is the post-central gyrus
Projection Fibers • We will concentrate on the efferent motor fibers • Four major divisions of the motor system have been identified • 1) the final common pathway (lower motor neuron system) • 2) the direct activation pathway (upper motor neuron system or pyramidal tract) • 3) the indirect activation pathway (extrapyramidal tract – direct contact with LMNs) • 4) the control circuits (basal ganglia and cerebellum – no direct contact with LMNs) • UMNs are part of the CNS, and LMNs are part of the PNS.
Projection Fibers • UMNs originate in the motor cortex and synapse onto cranial nerve nuclei in the contralateral brainstem (corticobulbar tract) or onto cells in the contralateral spinal cord (corticospinal tract) • LMNs originate in the cranial nerve nuclei (in which case they are known as cranial nerves) or in cells in the spinal cord (in which case they are known as spinal nerves). They synapse onto muscles. The junction between the LMN and the muscle is known as the motor end plate. • Cranial nerves innervate muscles of the head and neck, whereas spinal nerves innervate muscles of the limbs and trunk
Corticospinal Tract • Main pathway for nearly all voluntary muscle activity • Comprised of UMNs • It’s a bundle of axons, which changes names as it courses from cortex to muscles (corona radiata, posterior limb of the internal capsule, basis pedunculi) • This is a crossed pathway. At the level of the pyramids in the medulla, approx. 80-90% of the fibers in the tract cross to the other side of the brainstem; therefore, they descend in the opposite side of the spinal cord from where they originated.
Corticospinal Tract • Movement of one side of the body is controlled by the contralateral (opposite) side of the brain • Although the UMNs that originate in the pre-central gyrus are responsible for the initiation of voluntary motor activity, the UMNs that originate in the frontal lobe anterior to the pre-central gyrus do not initiate impulses. In fact, they act as suppressors or inhibitors of the LMNs. They prevent the LMNs from overdischarging in response to stimuli. If these inhibitory fibers are damaged, you end up with spasticity.
Corticobulbar Tract • Is comprised of UMNs • Originates in the motor cortex (lower third) • Crosses to the opposite side of the brain at various levels of the brainstem (midbrain, pons, medulla) • Innervates cranial nerve nuclei at various levels of the brainstem • Corticobulbar projections to most cranial nerve nuclei is bilateral, but corticobulbar projections to some cranial nerve nuclei is contralateral only
Projection Fibers • Thus, if UMNs are damaged, you get spasticity as well as not being able to initiate skilled motor movements • Spasticity = increased muscle tone. A Babinski sign signals the presence of UMN damage. Reflexes are exaggerated. • If LMNs are damaged, you end up with flaccid paralysis • Flaccidity = decreased muscle tone. Atrophy of muscles. Reflexes are diminished or absent.
Bilateral Cortical (UMN) Lesions – Spastic Dysarthria • Bilateral UMN lesions are likely to produce chronic dysarthria • The following can cause spastic dysarthria: stroke, CP, severe brain injuries, MS, encephalitis, and extensive brain tumors • Blood supply disruption – carotid artery system (e.g., MCA, ACA) • Spastic dysarthria is also called pseudobulbar dysarthria
Bilateral Cortical Lesions – Spastic Dysarthria • Strained-strangled phonation – associated with hyperadduction of the true and false vocal cords, and is characterized aerodynamically by elevated laryngeal airway resistance and subglottal pressure, and by reduced laryngeal airflow • Velopharyngeal dysfunction includes increased pharyngeal constriction; slow, sluggish velopharyngeal movement; and incomplete VP closure • Imprecise articulation
Unilateral UNM Lesions – Flaccid Dysarthria • Dysarthria in unilateral stroke is typically mild and temporary, and may co-exist with and be masked by aphasia or AOS • Imprecise consonant production was by far the most deviant speech feature in a retrospective study of 56 people with unilateral UMN dysarthria. Slow speaking and reduced oral movement rates were also found. • Physical findings of unilateral lower facial weakness and unilateral lingual weakness * (talk about why later) • Less common was vocal harshness and hypernasality. The neurologic bases of the phonatory and velopharyngeal features are unclear.
Unilateral and Bilateral LMN Damage: Flaccid Dysarthria • The LMNs to which we are referring are cranial nerves • Damage to one cranial nerve can result in flaccid dysarthria • Damage to multiple cranial nerves can result in flaccid dysarthria • The symptoms of flaccid dysarthria vary depending on which cranial nerves are damaged, and whether the damage is unilateral or bilateral • The following can cause flaccid dysarthria: stroke, CP, trauma, tumor, ALS, MG, Bell’s palsy, Guillain Barré
Lesions in the Area of Vertebrobasilar Circulation – Flaccid Dysarthria • Infarcts in the areas of the brain supplied by the vertebrobasilar system are less common than cortical infarcts, accounting for all CVAs • Brainstem strokes may result in flaccid paralysis of the speech muscles • Two major muscular abnormalities are weakness and hypotonia – seen in all movements of affected muscles (reflexive, automatic, or voluntary) • The salient perceptual speech characteristics are marked hypernasality coupled with nasal emission of air, continuous breathiness during phonation, and audible inhalation (stridor on inhalation)
Cranial Nerves • There are 12 pairs of cranial nerves • Cranial nerves are LMNs that originate in the cranial nerve nuclei (various levels of the brainstem) • Some cranial nerves are motor only, some are sensory only, and some are motor and sensory • The cranial nerves innervate the muscles of the jaw, face (including lips), pharynx, larynx, soft palate, tongue, and neck • The muscles affected are ipsilesional (i.e., the R cranial nerves innervate the R side of the body, and the L cranial nerves innervate the L side of the body)
Cranial Nerves • Six pairs of cranial nerves are important for speech • V – Trigeminal (sensory and motor) • VII – Facial (sensory and motor) • IX- Glossopharyngeal (sensory and motor) • X – Vagus (sensory and motor) • XI – Accessory (motor) • XII – Hypoglossal (motor) • Since most cranial nerve nuclei receive bilateral UMN innervation, unilateral UMN damage does not have a major deleterious effect on speech (with a few exceptions)
Trigeminal Nerve (V) • The trigeminal motor nucleus receives bilateral UMN input • The sensory fibers have 3 main branches (ophthalmic, maxillary, mandibular) • Motor to: • jaw (masseter, lateral and medial pterygoids) • temple (temporalis) • soft palate (tensor veli palatini) • larynx (mylohyoid and anterior belly of the digastric – both extrinsic muscles of the larynx) • middle ear (tensor tympani)
Trigeminal Nerve (V) • Functions • Cutaneous sensations (touch, pain, temperature) and proprioceptive sensations (awareness of posture and muscle movements) from the head, face, oral and nasal cavities, sinuses, teeth, anterior 2/3 of the tongue, anterior ½ of the pinna, external auditory meatus, and external surface of the TM • Mastication (jaw opening and closing, lateral movements of chewing) • Articulation (jaw opening and closing) • Flattening and tensing of the soft palate (which brings the soft palate to one side and prevents food from entering the nasal pharynx) • Prevents damage to the inner ear hair cells from loud noises when tensor tympani muscle contracts • Opens the eustachian tube
Trigeminal Nerve (V): Testing • Inspect the masseter and temporalis bulk • Palpate the masseter when the person bites • Observe the position of the jaw when the person is at rest • Ask the person to open and close the mouth • Evaluate the strength of jaw closure • Ask the person to move the jaw from side to side • Attempt to elicit the jaw jerk reflex (physician) • Test sensation by touching the person’s face with a cotton swab and asking if the person felt it • Ask the person about facial pain
Trigeminal Nerve (V) • Behaviors that Suggest Unilateral LMN Damage • Deviation of the jaw to the side of the lesion and an inability to force the jaw to the side opposite the lesion • Mildly reduced strength of the masticator muscles on the same side as the lesion • Reduced bulk of masseter and temporalis muscles (atrophy) on the side of the lesion • No major effects on speech • Ipsilateral loss of sensation to face, oral and nasal cavities, and other areas served by CN V • Trigeminal neuralgia (pain) on the same side of the face as the affected CN V
Trigeminal Nerve (V) • Behaviors that Suggest Bilateral LMN Damage • The jaw hangs open and cannot be closed, or moves slowly and with limited range • Reduced bulk (atrophy) of masseter and temporalis muscles on both sides of the face • Articulation is affected in a major way (labial and lingual articulatory movements are not accurate in place or manner) • Bilateral loss of sensation to face, oral and nasal cavities, and other areas served by CN V • Trigeminal neuralgia (pain) on both sides of the face
Trigeminal Nerve (V) • Behaviors that Suggest Unilateral UMN Damage (Input to CN V) • No real effect on speech because CN V receives bilateral UMN input • Behaviors that Suggest Bilateral UMN Damage (Input to CN V) • Limitation of jaw movement (opening and closing); mandible hangs low • Exaggerated jaw jerk reflex • Articulation is affected in a major way (vowels and labial and lingual consonants)
Facial Nerve (VII) • The motor cranial nerve nucleus that innervates the upper 1/3 of the face receives bilateral UMN input • The motor cranial nerve nucleus that innervates the lower 2/3 of the face receives primarily contralateral (unilateral) UMN input • Motor to: • Muscles of facial expression (orbicularis oculi, zygomatic, biccinator, orbicularis oris, platysma) • Middle ear (Stapedius) • Larynx (stylohyoid, posterior belly of the digastric – both are extrinsic muscles of the larynx) • Sensory to: • Sublingual, submandibular, and lacrimal glands • Taste receptors on the anterior 2/3 of the tongue
Facial Nerve (VII) • Functions • All movements of facial expression (e.g., wrinkle forehead, close eyes tightly, pull back corners of mouth) • Guards the middle ear by innervating the stapedius muscle, which acts to dampen excessive movement of the ossicles in the presence of a loud noise • Taste on the anterior 2/3 of the tongue
Facial Nerve (VII): Testing • Observe the person’s face at rest and note the symmetry • Ask the person to look up at the ceiling and note wrinkling of the forehead • Ask the person to close his/her eyes tightly and note wrinkling around the eyes • Ask the person to smile and note the symmetry • Ask the person to pucker his/her lips and note the symmetry • Ask the person to fill his/her cheeks with air, gently press on the cheeks, and note whether the person can maintain a lip seal • Does the person report that sounds are uncomfortably loud?
Facial Nerve (VII) • Behaviors that Suggest Unilateral LMN Damage • The entire side of the face ipsilateral to the lesion droops (e.g., forehead has no wrinkles, difficult to close eye, corner of mouth droops, flattened nasolabial fold). If the right CN VII is damaged, the right side of the face is affected. If the left CN VII is damaged, the left side of the face is affected. • Atrophy of the muscles on the side of the face ipsilateral to the lesion • Fasciculations of the peri-oral area and chin on the side of the face ipsilateral to the lesion • Speech is not negatively affected to any great extent. There may be some mild articulatory imprecision. • Ordinary sounds may be perceived as uncomfortably loud on the side ipsilateral to the lesion (hyperacusis) • Loss of taste from the anterior 2/3 of the tongue on the side of the tongue ispilateral to the lesion
Facial Nerve (VII) • http://www.uptodate.com/patients/content/images/neuropix/Bells_palsy_photos.jpg • http://thebarefootkitchenwitch.typepad.com/the_barefoot_kitchen_witc/images/2008/02/24/palsy.jpg • http://www.egms.de/figures/journals/cto/2005-4/cto000016.f4.png • http://www.ninds.nih.gov/disorders/bells/bells.htm
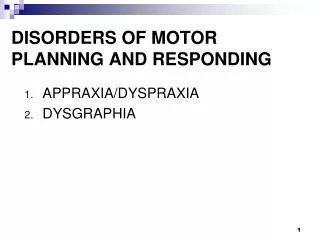
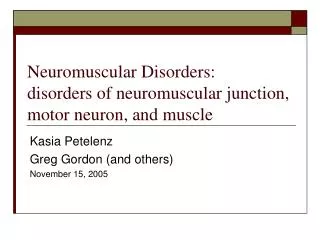
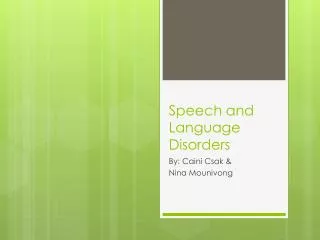
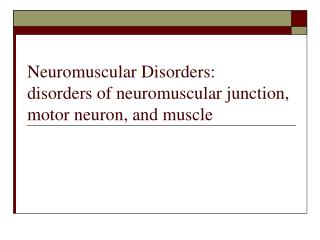
Facial Nerve (VII) • Behaviors that Suggest Bilateral LMN Damage • Both sides of the face are affected as described above • Hearing is affected bilaterally as described above • Taste is affected bilaterally as described above • Major difficulty producing labial and labiodental sounds • http://www.biomedcentral.com/1472-6815/4/3 • http://scienceblogs.com/purepedantry/2007/05/mobius_syndrome.php • http://www.ninds.nih.gov/disorders/mobius/moebius.htm
Bilateral Facial Weakness Before Tx for Herpes Zoster After Treatment
Mobius Syndrome Pre-surgery Post-surgery
Facial Nerve (VII) • Behaviors that Suggest Unilateral UMN Damage (Input to CN VII) • The lower 2/3 of the face on the side contralateral to the lesion will be affected (flattened nasolabial fold, corner of mouth droops) • Little effect on speech • Behaviors that Suggest Bilateral UMN Damage (Input to CN VII) • Paralysis of the upper and lower facial muscles on both sides of the face • Preservation of emotional expression even though there is paralysis of voluntary movements of the facial muscles • Major difficulty producing labial and labiodental sounds
Vagus Nerve (X) • Motor to: • Cardiac muscles • Smooth muscles of the esophagus, stomach, and intestine • Muscles of the pharynx and larynx • Muscles of the soft palate • Palatoglossal muscle of the tongue • Sensory to: • Mucosa of the pharynx • Inferior surface of the epiglottis • Trachea, bronchi, esophagus, stomach, intestines • Mediates pain input and stretch afferent feedback from pharyngeal and laryngeal muscles • The nucleus ambiguus of CN X receives bilateral innervation
Vagus Nerve (X) • Functions • Regulation of cardiovascular, respiratory, and gastrointestinal functions • Taste sensation from the pharyngeal area • Controls muscles of the larynx, pharynx, and soft palate for phonation, swallowing, and resonance, and for opening the respiratory pathway • Motor fibers originate from the posterior 2/3 of the nucleus ambiguus. These fibers give rise to the pharyngeal nerve, the superior laryngeal nerve, and the recurrent laryngeal nerve (all branches of CN X).
Vagus Nerve (X) • Pharyngeal nerve • Supplies the three pharyngeal constrictor muscles • Supplies all soft palate muscles except the tensor veli palatini • Superior laryngeal nerve • Supplies the cricothyroid muscle (an intrinsic muscle of the larynx that lengthens the vocal folds for pitch adjustments) • Sensory to the mucous membrane as far down as the vocal cords • Recurrent laryngeal nerve • Supplies all RIML (remaining intrinsic muscles of the larynx) • The left and right recurrent laryngeal nerves take different paths. The L hooks under the aortic arch near the heart.
Vagus Nerve (X): Testing • Observe the soft palate at rest and when the person says, “Ah” (multiple short productions) • Elicit a gag reflex • Laryngoscopy to visualize the vocal folds • Ask the person to phonate and prolong a vowel sound • Ask the person to raise and lower the pitch of a prolonged vowel or sing up and down a scale • Listen to the person during conversation • Ask the person to count to 300 (speech stress test)
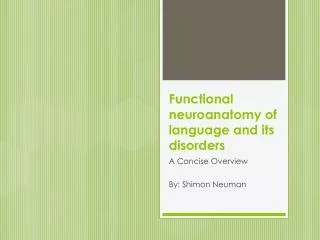
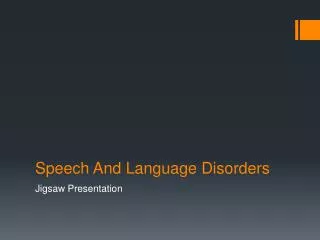
Vagus Nerve (X) • Behaviors that Suggest Unilateral LMN Damage • Palate droops on side ipsilateral to lesion; mild hypernasality • http://www.scielo.br/img/revistas/anp/v64n3a/a15fig01.gif • Vocal fold is paralyzed on same side as lesion; breathy and/or hoarse voice; diplophonia • Weak pharynx on same side as lesion; swallowing difficulty • Behaviors that Suggest Bilateral LMN Damage • This state of affairs is often not compatible with life (respiratory centers in this area of the brainstem) • Palate droops bilaterally; severe hypernasality • Bilateral vocal fold paralysis (flaccid); severe breathy voice; inhalatory stridor • Weak pharynx bilaterally; severe swallowing difficulty
Unilateral VF Paralysis(Damage to CN X) Abducted Position (R L) Adducted Position (R L)
Vagus Nerve (X) • Behaviors that Suggest Unilateral UMN Damage (Input to CN X) • minimal to no effect on phonation, resonance, or swallowing because of bilateral innervation • Harsh voice quality • Behaviors that Suggest Bilateral UMN Damage (Input to CN X) • Paralysis of vocal folds in the paramedian position; spasticity of VFs • Strained-strangled phonation, hypernasality • Swallowing difficulty
Hypoglossal Nerve (XII) • The nucleus of CN XII receives bilateral innervation with one exception: the cells serving the genioglossus muscle (the largest muscle of the tongue – protrudes and retracts tongue, and elevates hyoid bone) receive only contralateral UMN input • CN XII innervates all intrinsic muscles of the tongue and 3/4 extrinsic muscles of the tongue (genioglossus, hypoglossus, styloglossus) • Functions: all movements of the tongue • Shortening, concaving, narrowing, elongating, flattening • Protrusion, drawing the tongue upward and backward, retraction and depression • The genioglossus participates in phonation (it elevates the hyoid bone)
Hypoglossal Nerve (XII): Testing • Observe the tongue at rest • Ask the person to stick out the tongue • Ask the person to move the tongue from side to side • Ask the person to elevate and lower the tongue tip • Ask the person to protrude and retract the tongue • Ask the person to lick his/her lips