Download
1 / 17
210 likes | 1.57k Views
DYSPHAGIA (DIFFICULTY SWALLOWING). **********************************************************. DYSPHAGIA SIGNS AND SYMPTOMS. Coughing is a reflex, its’ the body’s response to clear the airway Vomiting—is due to esophageal dysfunction Drooling—signs of dysphagia

E N D
DYSPHAGIA(DIFFICULTY SWALLOWING) **********************************************************
DYSPHAGIASIGNS AND SYMPTOMS • Coughing is a reflex, its’ the body’s response to clear the airway • Vomiting—is due to esophageal dysfunction • Drooling—signs of dysphagia • Wet Vocal Cords—happens after choking • Rails—a metal sound a medical person hears with a stethoscope in a persons lungs that may be congested • Refusal behavior—preferences to certain foods—due to the feeling of choking with certain foods • Fever (high) can or may lead to aspiration • Pocketing food in mouth • Weight loss • Gaging Throat clearing Multiple swallows • Excessive time to swallow
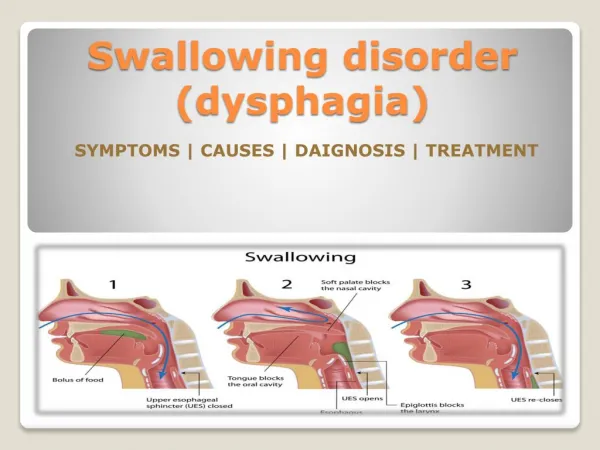
DYSPHAGIAMECHANISMS • When swallowing you can feel the larynx move forward • Place 2 or 3 of your fingers to your throat and swallow—feel the movement pushing against your finger? This is the larynx doing its part in the swallowing process to move food down the esophagus • Its takes approximately 20 seconds to swallow
DysphagiaCauses of Dysphagia • Developmental Delay • Seizure Disorder • Motor deficits—CP, CVA, TBI, neuromuscular disorders • Cognitive Impairment—MR, CVA, TBI, dementia • Cancer of the head or neck • Meds that: (sedate, decrease saliva production)
Dysphagia Abnormal Pathology • Piecemeal deglutination—many tiny swallow • Premature spillage—food spills into the esophagus before swallowing • Pooling in sinuses—food pools in these cavities eventually will clear with swallowing • Penetration—to the level of the vocal cords • Silent aspiration—food may pass the larynx, pass the pharynx no coughing noted (usually unaware) • Barrett’s Esophagus—out pocketing of esophagus bacteria can collect & predispose area to cancer (precancerous) • Stricture– scarring- due to trauma, Eg. Induced vomiting (bulemina) eventually esophagus will reduce in size
DysphagiaFYI • Average person swallows 2000 times a day • Our population is at high risk from death from aspiration pneumonia • History of “Reflux” will create weaker sphincters which may again lead to aspiration pneumonia • Aspiration pneumonia is when someone swallows and instead of the substance going down the esophagus it goes down the windpipe into the lungs and causes an infection which leads to pneumonia • Consumers with severe scoliosis are at a higher risk
Dysphagia Health Impact • When a person is diagnosed with Dysphagia they become a higher risk for the following: • Poor absorption of mediations • Dehydration • Aspiration Pneumonia • Poor eating habits • Fear of aspiration (choking) • Reflux—age and or anatomy as contributing factors, if untreated can cause significant problems
DysphagiaDocumentionDirect Care Staff • It is important to record when consumers refuse to eat what is on their diet plan, and record what they eat. Make sure you offer what is on their meal plan at every meal. • Diet adjustments will take time. Eg. “Prader Willi” (a condition when the brain can not register with the stomach that the person is full) • You may help at meal time by deferring them with a activity • If you notice a consumers is starting to exhibit some signs and symptoms of difficulty swallowing. You will need to make good documentation and notify the nurse and their home what you are observing.
DysphagiaHigh Risk Foods • Certain foods can often be potential hazards to someone with Dysphagia or even very young children if not properly prepared • Eg. Hotdogs, grapes, popcorn, peanut butter on white bread, candy, nuts, raisins, raw fruit/veggies Note: At meal-time talking or distractions away from eating can create a potential choking situation for someone with Dysphagia, it is important to create a calm atmosphere for meal-time Make sure if the consumer has a habit of eating to fast to remind them to slow-down Positioning: Pelvis as a core base of support (have buttdocks to the back of the sit) Lock in legs next 90 90 90 degree angle of body Trunk in medline External supports as needed
DysphagiaTube Feeders • Make sure the person you are feeding of giving liquids via G-tube is sitting up during and after feeding to prevent choking and aspiration • If you are having difficulty with the food going down the tube you may reposition the consumers or place a pillow on their side to help the procedure go more smoothly • Consumers who have a G-tube have been diagnosed with some degree of difficulty swallowing • FYI: G-tube feeders if given not given oral care within 5 years will loose their ability to eliminate secretions after instilling the tube • To help stimulate salvia production 2 foods that can help assist are cotton candy and lolly-pops. These are pleasure foods.
DysphagiaAdaptive Equipment • There are many utensils that can help a person stay as independent with self-feeding as possible. A few are listed below: • Nosey cup • 3 section plate • Kennedy cup (designed to prevent spillage) • Infant spoons (help fast eaters to slow-down) • Weighted utensils help clients with tremors • Cuff handle adheres to hand for self-feeders • Pizza knife (as a cutting tool) • Note: You can use foam hair rollers on utensils to create a larger circumference for better control for self-feeders
DysphagiaTeam Members • The following people can make-up a team for a consumer who has Dysphagia: • Oral Motor / Dysphagia Specialist—Occupational therapy or speech • MD • Dietician • Physicial Therapist • Caregiver (Direct care) • The individual
DysphagiaFood ConsistencesADA National Dysphagia Diet • Level 1 Pureed • Level 2 minced 1/8” • Level 3 ground ¼” • Level 4 chopped ½” • Level 5 modified regular • Liquid Textures: • Thin—almost everything we drink • Nector—tomato juice / sauce consistency • Milkshake—McD’s consistency • Pudding—fed by a spoon • Thicket: • Thicket is a thickening agent to help make liquid foods easier to swallow per doctors orders • Start with the recipe on the can per doctors orders • Whisk versus stir into food • It will thicken over time do not allow to sit, use immediately
DysphagiaHead Control Techniques • Use only APPROVED head control techniques such as: • Chin lift—thumb on chin; index finger under chin pull down • Chin or cheek cup—form a“C” between thumb & index finger place on each side of the cheeks and press slightly • Crowning techniques—open hand place the palm at the top of the forehead push up slightly (these techniques will help with feeding or giving medications) • Note: The above techniques have been approved to use in feeding
DysphagiaDependent / Independent Feeding • Dependent Feeding: • Fed by caregiver due to physical inability, safety issues, • Note: ½ tsp of solid to 1 sip of liquid or 1 bite / sip 1 swallow • Alternate solids with liquids—5 bites to 1—2 sips ratio • Independent Feeding: • Is assisted and supervised, monitoring consumers skills as they eat • Visually Impaired Diner: • Consistent place a the table • Place setting by the “Clock” Eg. Meat at 12:00, Potato at 3:00 • Hands as help • The Quiz is next…..when your done taking the quiz, you may put it in the nurse’s box.
DysphagiaQuiz • 1. List 3 signs that may indicate a person is having a swallowing problem. __________________________________________________________ __________________________________________________________ __________________________________________________________ 2. What is dysphagia?__________________________________________ __________________________________________________________ 3. Name 2 things that can contribute to dysphagia ________________________ __________________________ 4. List 4 foods that may contribute to choking ________________________ __________________________ ________________________ __________________________
DysphagiaQuiz • 5. List 2 “pleasure foods” to help stimulate salvia production • 6. List 2 team members who would assist in the care of someone with dysphagia. _______________________ ___________________________ 7. Describe what (Thicket) is?______________________________________________ ____________________________________________________________________ 8. Name 2 types of consistency food can be prepared at. ___________________________ __________________________________ 9. When you aspirate food, where does it go?__________________________________ 10. What will adaptive equipment help the individual be able to do? ____________________________________________________________________ ____________________________________________________________________ 11. When caring for a person with a G-tube, you should leave the tubing out so you can see it? True or False (circle the right answer) Explain why____________ ____________________________________________________________________