Download
1 / 43
430 likes | 746 Views
Pediatric Diseases Requiring Respiratory Care. Mary P. Martinasek BS,RRT Director of Clinical Education Hillsborough Community College. ARDS. Acute Respiratory Distress Syndrome Mortality 60% Pathophysiology VQ mismatch Pulmonary hypertension Reduced compliance Pulmonary infiltrates.

E N D
Pediatric Diseases Requiring Respiratory Care Mary P. Martinasek BS,RRT Director of Clinical Education Hillsborough Community College
ARDS • Acute Respiratory Distress Syndrome • Mortality 60% • Pathophysiology • VQ mismatch • Pulmonary hypertension • Reduced compliance • Pulmonary infiltrates
ARDS • Direct or Indirect Injury • Four distinct phases • I - dyspnea and tachypnea • II - 12 - 24 hours,alveolar damage, infiltrate on CXR • III - leaky alveolar capillary membranes • IV - progressive respiratory failure
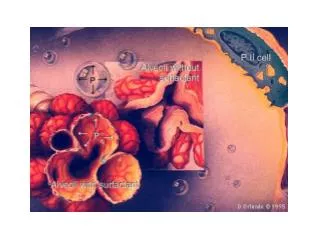
ARDS • Signs and Symptoms • Initially = crackles, dyspnea, retractions, grunting, RR • Then compliance worsens, adventitious sounds more apparent, Vd • Treatment • Supporting the lungs • Surfactant • Nitric Oxide • lung edema • PGE ?
Asthma • Most common pediatric disease Hyperreactive Airway • Etiology unknown • Pathophysiology • 2 phases • Early acute allergic phase • Spasm of bronchial smooth muscles • Late Inflammatory phase • Hypersecretion of mucus • Goblet cell hyperplasia • Smooth muscle hypertrophy • Influx of inflam. Cells into the airway
Late Phase reactions lead tosmall airway obstruction air trapping auto peep VQ mismatch More negative intrapulmonary pressure to maintain Tidal Volume
Precipitating Factors • Allergens • Outdoor irritants • Indoor irritants • Exercise • Viral infections • Foods • Emotions • Aspirin and related drugs
Asthma • Signs and Symptoms • Wheezing, RR, HR • SOB • Four stages according to ABG • Treatment • Avoid precipitating factors • Keep PaO2 greater than 55 torr • Heli-ox (80:20) (70:30) • Bronchodilators and Steroids
Asthma cont. • Moderate attack: Audible wheezing • No wheeze may indicate severe obstruction • Patient with cyanosis and diaphoresis must be treated immediately • Pulsus Paradoxus
Asthmatic on vent • PIP due to airway resistance • PIP generated in ET tube and airways, not the alveoli • Goal = Keep plateau 35-40 cmH20 • Do not flow to PIP • Result would be I:E change and auto peep
Asthmatic Meds • Sympathomimetic works on small peripheral bronchioles • Parasympatholytic works on large airways • Sympathomimetics = Albuterol, Xopenex • Parasympatholytic = Atrovent
Asthma Meds cont. • Corticosteroids = suppress the release of inflammatory mediators • Example = Flovent, Beclovent • Prevention of Mast cell degranulation • Intal and Tilade • Block leukotriene receptors (prophylaxis) • Singulair, Accolate (po)
Cystic Fibrosis • Autosomal Recessive disease • Observable by three clinical disorders • Pulmonary disease • Pancreatic insufficiency • Elevated sweat chloride concentrations • Ionotrophic testing - pilocarpine • Manifests itself as dehydration of secretions
CF • Colonization infection inflammation airway obstruction pulmonary dysfunction • CF affects every organ in the body that has epithelial surface • Lung, pancreas, intestines
Cystic Fibrosis • Pathophysiology • Pancreatic fibrosis • Pulmonary disease • Pseudonas • S. Aureus • Diagnosis • Sweat Chloride Test • Greater than 60 meq/l • Treatment • O2, aerosolized abx,bronchodilators, CPT, flutter valve, nutrition, pancreatic enzyme
Neuromuscular Disorders • Muscular Dystrophies • Largest group of muscle diseases that affect children • Progressive symmetrical weakness and wasting of skeletal muscles • Affect the muscles of respiration in four ways • Defects in the muscle itself • Defect in the transmission of nervous impulses to the muscles • Defect in the peripheral motor and sensory nerves • Defect in the CNS • Duchenne muscular dystrophy • Most severe and most common • (Pseudohypertrophic)
Neuromuscular Disorders • Guillian-Barre Syndrome (Infectious Polyneuritis) • Linked to mono, hepatitis, influenza, CMV • Tetanus • Preventable = vaccinations • Acquired through wound in skin • Botulism • Ingestion of food contaminated with Clostridium botulinum • Improperly prepared home-canned foods • Weakness, dizziness, headache, vomiting • Respiratory muscle paralysis • Treatment = botulism antitoxin
Neurologic Disorders • Myasthenia Gravis - Tensilon Test • Spinal Cord Injuries - • 3 goals in management • Preservation of neurologic function • Maximization of neurologic recovery • Prevention of intercurrent nonneurologic complications • Head Injury • Primary and secondary injuries • Near Drowning= survival of victim of submersion for greater than 24 hours
Reyes Syndrome • Life threatening illness causing liver function deterioration and encephalopathy of the brain • Associated with chicken pox, flu and aspirin ingestion during a viral illness • Signs= listlessness, loss of energy, drowsiness, irritability, aggresiveness, confusion, irrational behavior • SGOT and SPGT enzyme levels
Lung Diseases • Pneumonia • RSV, Parainfluenza, Strep, Staph, H. flu • Bacterial = sudden onset, fever • Viral = preceded by common cold, low grade temp. • Diagnosis = CXR, blood cultures, CBC • Bronchiolitis - most common cause of lower respiratory infections in young children • Viral = RSV or Parainfluenza virus • Fall and Winter months • Diag. - NP cultures + PMH • TX - O2, CPT?, Ribavirin?, Synagist, Theophylline
Upper Airway Diseases • Epiglottitis = supraglottic swelling • 80% H Flu • 2 - 6 yrs. • Drooling, Tripod position • Tx = antibiotics • Thumb sign on CXR • Croup (Laryngotracheobronchitis) = Subglottic swelling • Parainfluenza, RSV • Steeple sign on CXR • TX = cool mist, racemic epi, steroids
Upper Airway Diseases • Aspiration Syndrome • FBA = Foreign body aspiration • Severity depends on size and location of obstruction • Sign = Cough and gag then stridor and wheeze • CXR = Flexible bronchoscopy under anesthesia • Complications = air leak, pneumonia
Inhalation • Smoke Inhalation - COHb levels @ 20-30% • Tx with 100% O2 • Half life of CO is 6 hours
SIDS • Sudden Infant Death Syndrome • Accounts for highest number of deaths in infants less than one year • Diagnosis made with autopsy • Back to Sleep program • Factors that increase the risk of SIDS • Use of natural fiber mattresses • Swaddling • Recent illness • Use of heating in room