Download
1 / 26
260 likes | 647 Views
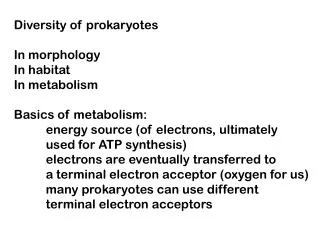
Case Study in RRT in In Born Error of Metabolism. Timothy E. Bunchman Pediatric Nephrology & Transplantation VCU School of Medicine tbunchman@mcvh-vcu.edu pcrrt@aol.com www.pcrrt.com. In Born Error of Metabolism. 2.9 kg infant presents at 48 hours of life with lethargy.

E N D
Case Study in RRT in In Born Error of Metabolism Timothy E. Bunchman Pediatric Nephrology & Transplantation VCU School of Medicine tbunchman@mcvh-vcu.edu pcrrt@aol.com www.pcrrt.com
In Born Error of Metabolism • 2.9 kg infant presents at 48 hours of life with lethargy. • Child is afebrile, BP is 75/40, HR of 130 BPM, RR of 50 BPM • On exam “floppy” infant with poor neurologic tone
In Born Error of Metabolism • Normal laboratory data shows of • H/H of 15/45; Cr of 0.9 mg/dl (maternal) , K of 4.3 mq/dl, Ca of 9.5 mg/dl, Phos of 6.0 mg/dl (nl) • Abnormal laboratory data shows • CO2 of 14 mg/dl and a ammonia of 1533 micromls/l (nl < 40)
30 newborns at OBG: OA 14 pts : 8 PA, 4 MMA, 1 HMG, 1 IVA UCD 16 pts : 3 CPS, 4 OTC, 5 AL, 3 AS,1 HHH Dionisi-Vici et al. J Inher Met Dis2003
“SMALL MOLECULES” DISEASES INDUCING CONGENITAL HYPERAMMONEMIA. • INCIDENCE • Overall: 1:9160 • Organic Acidurias: 1:21422 • Urea Cycle Defects: 1:41506 • Fatty Acids Oxidation Defects: 1:91599 • AGE OF ONSET • Neonate: 40% • Infant: 30% • Child: 20% • Adult: 5-10% (?)Dionisi-Vici et al, J Pediatrics, 2002.
KEY POINTS FACING TO A HYPERAMMONEMIC NEWBORN • hyperammonemia is extremely toxic to the brain (per se or through intracellular excess glutamine formation) causing astrocyte swelling, brain edema, coma, death or severe disability, thus: • emergency treatment has to be started even before having a precise diagnosis since: • prognosis mainly depends on coma duration
PROGNOSIS OF HYPERAMMONEMIC COMA IS DEPENDENT ON COMA DURATION. from Msall M et al, N Eng J Med 1984.
TREATMENT of SEVERE NEONATAL HYPERAMMONEMIA IMMEDIATE MEDICAL THERAPY NO RESPONSERESPONSE DIALYSIS MAINTAINANCE MEDICAL THERAPY + REFEEDING IMMEDIATE DIALYSIS + MEDICAL THERAPY MAINTAINANCE MEDICAL THERAPY + REFEEDING ?
Pharmacological treatment before having a diagnosis AIMS precursorscatabolismanabolism • stop protein • caloric intake 100 kcal/kg • insulin …and • endogenous depuration • arginine 250 mg/Kg/2 hrs + 250 - 500 mg/Kg/day • carnitine 1g i.v. bolus 250 - 500 mg/Kg/day • vitamins (B12 1 mg,biotin 5-15 mg) • benzoate 250 mg/Kg/2 hrs + 250 mg/Kg/day or • peroral phenylbutyrate (only after UCD diagnosis) Picca et al. Ped Nephrol 2001
urea PD CRRT HD time ammonium? generation rate clearance [C]
RRT intervention • Child was electively intubated for airway protection • Foley catheter placed for use for urine collection and accurate I/O • Na Pheyacetate, Na Benzoate, Arginine Cl, Carnitine were all begun once urine and plasma amino and organic acids obtained.
RRT intervention • A 7 Fr 10 cm MedComp “softline” duel lumen vascular access placed • HD begun using a blood prime and a Phoenix (Gambro) • BRF of 70 mls/min (~ 22 mls/kg/min) • DFR of 500 mls/min with a physiologic K and Phos bath • Ammonia levels collected at 1 hr intervals
Ammonia Clearance HD Begins 1800 HD Ends 1600 1400 1200 Ammonia (micromol/l) 1000 800 600 400 200 0 1 2 3 5 7 11 15 17 19 Time (hours)
RRT intervention • At 2 hours of HD the ammonia was ~ 200 micromls/l and HD was exchanged for CVVHDF (Gambro Prisma M 60 membrane) using the same vascular access • A blood prime bypass maneuver was performed • Replacement rate of 2 liters per hour and a dialysate rate of 1 liter per hour • (HD clearance was 30 l/hr now decreased to 3 l/hr)
Ammonia Clearance HD Begins HF Ends 1800 HD Ends 1600 HF Begins 1400 1200 Ammonia (micromol/l) 1000 800 600 400 200 0 1 2 3 5 7 11 15 17 19 Time (hours)
RRT intervention • A few practical comments • Ammonia is non-osmolar so no risk of dialysate disequilibrium exists • In Born Error of metabolism infants appear to be polyuric so keeping them intubated and keeping them “wet” is important
PHARMACOLOGICAL TREATMENT DIAGNOSIS NO RESPONSE RESPONSE RE-FEEDING DIALYSIS TREATMENT of NEONATAL HYPERAMMONEMIA HOSPITALIZATION
PD patients 180 160 140 120 100 NH4p (percent of initial value) 80 60 40 20 0 0 5 10 15 20 25 Time (hours)
CAVHD patients 100 80 60 40 20 0 0 10 20 30 40 50 60 100 CVVHD patients 80 NH4p (percent of initial value) 60 40 20 0 0 10 20 30 40 50 60 HD patients 100 80 60 40 20 0 0 10 20 30 40 50 60 Picca et al. Ped Nephrol 2001 TIME (hours)
AMMONIUM CLEARANCE AND FILTRATION FRACTION USING DIFFERENT DIALYSIS MODALITIES. Picca et al., 2001
Drug clearance • Where as ammonia is a small molecular wt compound Na Phenylacetate and Na Benzoate are also small, non protein bound • So will your therapy clear the drug?
Conclusion • Hyperammonemia of the new born is a medical and dialytic emergency • Immediate institution of medical therapy is needed and a early decision of RRT institution is needed
Conclusion • PD has little to offer in this disease • HD is the preferred modality and prevention of the rebound can occur by transitioning HD to HF • With RRT monitor K and Phos closely to avoid loss of these electrolytes during the RRT