Download
1 / 33
1.48k likes | 7.85k Views
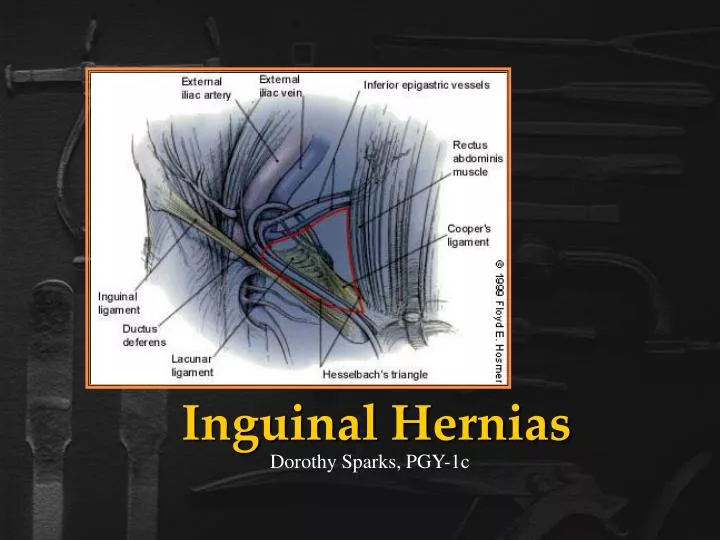
Inguinal Hernias. Dorothy Sparks, PGY-1c. Historical Hernias. Hernias have been documented throughout history with varying success at either reduction or repair. Trusses & Techniques. Anatomic Considerations.

E N D
Inguinal Hernias Dorothy Sparks, PGY-1c
Historical Hernias Hernias have been documented throughout history with varying success at either reduction or repair.
Anatomic Considerations • The inguinal region must be understood with regard to its three-dimensional configuration • A knowledge of the convergence of tissue planes is essential • If repairing the hernia laparoscopically, the anatomy must be well understood from the peritoneal surface outward • There is a considerable amount of anatomic variability with regard to: • Size and location of the hernia • Degree of adipose tissue
Anatomic Considerations • The surgeon must also be aware of the precise location of the: • Femoral nerve • Genitofemoral nerve • Lateral femoral cutaneous nerves
Pelvic & Inguinal Anatomy Both the ilioinguinal nerve and the genitofemoral nerve traverse the usual hernia-repair operative field. The femoral vein also runs just deep to the inguinal floor laterally.
Myopectineal Orifice of Fruchaud The MPO is bordered: • Above by the arching fibers of the internal oblique and transversus abdominus Muscles, • Medially (towards the center or to the right) by the Rectus Abdominus Muscle and its fascial Rectus Sheath • Inferiorly by Coopers Ligament, and • Laterally by the Ileopsoas Muscle • Running diagonally thru the MPO is the inguinal ligament
Hesselbach's triangle Boundaries: Medial: Rectus abdominis muscle medially, Inferiorly: Inguinal ligament Laterally: Inf. Epigastrics
Diagnosis • The patient usually presents (for groin hernia) with the complaint of a bulge in the inguinal region • They may describe minor pain or vague discomfort associated with the bulge • Extreme pain usually represents incarceration with intestinal vascular compromise • Paresthesias may be present if inguinal nerves are compressed
Diagnosis • Physical exam • The patient should be standing and facing the examiner • Visual inspection may reveal a loss of symmetry in the inguinal area or bulge • Having the patient perform valsalva’s maneuver or cough may accentuate the bulge • A fingertip is then placed in the inguinal canal; Valsalva maneuver is repeated • Differentiation between indirect and direct hernias at the time of examination is not essential
Diagnosis • Physical exam • Incarcerated hernias sometimes can be reduced manually • Gentle continuous pressure on the hernial mass towards the inguinal ring is generally effective (Trendelenburg)
Nyhus Classification • Type I:Indirect inguinal hernia Internal inguinal ring normal (simple pediatric hernia) • Type II:Indirect inguinal hernia Internal inguinal ring dilated but posterior inguinal wall intact (inferior deep epigastric vessels not displaced)
Nyhus Classification • Type III:Posterior wall defect • A. Direct inguinal hernia • B. Indirect inguinal hernia- internal inguinal ring dilated (massive scrotal or sliding hernia) • C. Femoral hernia • Type IV: Recurrent hernia • A. Direct • B. Indirect • C. Femoral • D. Combined
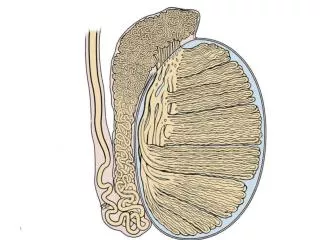
Inguinal Hernia • Indirect inguinal hernia • Is a congenital lesion • Occurs when bowel, omentum or other abdominal organs protrudes through the abdominal ring within a patent processus vaginalis • If the processus vaginalis does not remain patent an indirect hernia cannot develop • Most common type of hernia
Indirect Hernia Route Note: The hernia sac passes outside the boundaries of Hesselbach's triangle and follows the course of the spermatic cord.
Inguinal Hernia • Direct inguinal hernia • Proceeds directly through the posterior inguinal wall • Direct hernias protrude medial to the inferior epigastric vessels and are not associated with the processus vaginalis • They are generally believed to be acquired lesions • Usually occur in older males as a result of pressure and tension on the muscles and fascia
Direct Hernia Route Note: The hernia sac passes directly through Hesselbach's triangle and may disrupt the floor of the inguinal canal.
Incidence • Approximately 700,000 hernia repairs are performed as an outpatient procedure each year • Approximately 75% of all hernias occur in the inguinal region • Approximately 50% of hernias are indirect inguinal hernias • A vast majority occur in males • Hernias more commonly occur on the right side
Causes of Groin Hernias • Divided into two categories:congenital & acquired defects • Congenital factors are responsible for the majority of groin hernias • Prematurity and low birth weight are significant risk factors • Direct hernias are attributed to the wear and tear stresses of life • Groin hernias have been demonstrated to occur more frequently in smokers than nonsmokers especially women
Specific Surgical Procedures • Lichenstein (Tension Free) Repair • McVay (Cooper’s Ligament) Repair • Shouldice (Canadian) Repair • Laproscopic Hernia Repair • Bassini Repair
Bassini Repair • Is frequently used for indirect inguinal hernias and small direct hernias • The conjoined tendon of the transversus abdominis and the internal oblique muscles is sutured to the inguinal ligament
McVay Repair • AKA: Cooper’s ligamentRepair • Is for the repair of large inguinal hernias, direct inguinal hernias, recurrent hernias and femoral hernias • The conjoined tendon is sutured to Cooper’s ligament from the pubic cubicle laterally
McVay Repair Note: This repair reconstructs the inguinal canal without using a mesh prosthesis.
Shouldice Repair • AKA: Canadian Repair • A primary repair of the hernia defect with 4 overlapping layers of tissue. • Two continuous back-and-forth sutures of permanent suture material are employed. The closure can be under tension, leading to swelling and patient discomfort.
Lichtenstein Repair AKA: Tension-Free Repair One of the most commonly performed procedures A mesh patch is sutured over the defect with a slit to allow passage of the spermatic cord
Lichtenstein Repair Note: Open mesh repair. Mesh is used to reconstruct the inguinal canal. Minimal tension is used to bring tissue together.
Laparoscopic Hernia Repair • Early attempts resulted in exceptionally high reoccurrence rates • Current techniques include • Transabdominal preperitoneal repair (TAPP) • Totally extraperitoneal approach (TEPA)
Laparoscopic MeshRepair Note: Viewed from inside the pelvis toward the direct and indirect sites. A broad portion of mesh is stapled to span both hernia defects. Staples are not used in proximity to neurovascular structures.