Download
1 / 18
180 likes | 355 Views
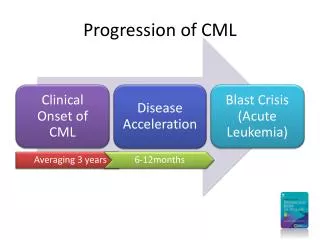
CML Registry. Joerg Hasford, MD Ludwig-Maximilians University Munich, Germany. Speaker disclosed relations to Novartis. European CML Registry. M. Baccarani Italy J. Guilhot France B. Simonsson Sweden Joerg Hasford Germany.

E N D
CML Registry • Joerg Hasford, MD • Ludwig-Maximilians University • Munich, Germany Speaker disclosed relations to Novartis
European CML Registry M. Baccarani Italy J. Guilhot France B. Simonsson Sweden Joerg Hasford Germany IBE Department of Medical Informatics, Biometry and Epidemiology, Ludwig-Maximilians-Universität München Email: has@ibe.med.uni-muenchen.de
Structure • Objectives • Clinical Data • Epidemiological data • Treatment survey • Discussion • Conclusions
European CML RegistryOBJECTIVES Clinical • to develop and validate • a comprehensive prognostic model which allows to optimise individual treatment choices • in particular a prognostic model for treatment with imatinib • to evaluate • the impact of therapeutic drug monitoring, pharmacokinetics and patients’ compliance during the course of CML • the sequelae of discontinuation of treatment after complete cytogenetic remission (CCR) • the mechanisms and sequelae of imatinib failure
European CML RegistryOBJECTIVES Epidemiological • to collect baseline and treatment data of representative samples of CML patients of all European countries • to estimate the incidence of CML stratified for age, sex and region • to evaluate the medical management of CML patients using the ELN recommendations (Blood 2006;108:1809-20)
European CML RegistryOBJECTIVES General • to promote quality controlled molecular monitoring • to foster continued medical education and spread of excellence • to develop and keep updated a core data set for CML • to provide a platform for the expedited evaluation of new treatments • to promote European trials, meta-analyses and pooled data analyses
Data provided by the cooperating study groups Study Type Treatment options n I - ICSG CML 21 Phase II imatinib 800 mg 82 I - ICSG CML 22 Phase III imatinib 400 mg vs 800 mg 117 I - ICSG CML 23 Phase II imatinib 400mg 365 German gr. CML IVPhase II 4 arms imatinib treatment 904 E- CML/PETHEMA Phase III imatinib treatment 200 E - RELMC Registry any imatinib therapy 318 Nordic CML001 Phase III imatinib 400mg vs 800mg 103 Nordic CML002 Phase II imatinib 400 mg vs 400mg+PEG-IFN 50 ROM – Registry Registry any imatinib therapy 33 F - Spirit Phase III 4 arms imatinib treatment 370 PL - Registry Registry any imatinib therapy 267 Total 2809
Inclusion criteriaaccording to the CML Guidelines (Baccarani et al. Blood 2006) • Patients with Philadelphia positive or BCR/ABLpositiveCML in early chronic phase* treated with a tyrosine kinase inhibitor (mainly imatinib) • No age limitations • 2062** of 2809 patients were included in the registry • * Early chronic phase: patients in chronic phase and therapy begin with tyrosine kinase inhibitors within six months after diagnosis. • ** the number of accepted patients may decrease or increase slightly as baseline and follow up data are not available for all patients yet; therefore inclusion criteria are sometimes still missing.
Study data expected for the European CML-Registry Cooperation with the Austrian study group, the OSHO study group, a Russian study group, and the CAMELIA / INFINITY are in progress.
European CML-Registry: Baseline characteristics
European CML-Registry: Results Cytogenetic remission at month 12 complete partial minor minimal no response Registry* (n=802)75.4 % 13.0 % 3.6 % 3.9 % 4.1 % Female* (n=325) 76.6 % 10.8 % 3.1 % 4.6 % 4.9 % Male* (n=477) 74.6 % 14.5 % 3.9 % 3.4 % 3.6 % IRIS 69.0 % 16.0 % All patients treated with imatinib 400 mg with or without co-medication, and data included if t > 2 months. * data was available of the German, Italian and Nordic study group
CML-Incidence and treatment survey Joerg Hasford, Martin Tauscher Population: Bavaria ~12.4 million inhabitants Data base: The Bavarian Association of SHI-Accredited Physicians (KVB) Coverage: 83.5% of outpatient care in Bavaria (10.4 million) Time: 2003 - 2005 CML case definition: ICD C92.1 Chronic myeloid leukemia and treatment with either imatinib, interferon alpha, hydroxyurea or busulfan,treatment > 1 year
Results - Incidence 2004 201 new CML-patients → 1.93 / 100,000 / year 2005 187 new CML-patients → 1.80 / 100,000 / year Age (median) Male: 50.7 % 63 years Female: 49.3 % 65 years Population (SHI): 10,387,207
Incidence of CML - International Data (WSP) Bavaria UK 1 UK 2 Women 1.06 0.47 0.67 Men 1.36 0.72 1.00 All persons 0.83 Incidence per 100’000 1Mc Nally RJQ et al. Hematol Oncol 1997;15:173-189. 2 Phekoo KJ et al. Hematologica 2006;91:1400-1404.
Conclusions • The European CML Registry has been successfully established. • The cytogenetic remission rates 12 months after treatment initiation with imatinib 400 mg/d have been successfully reproduced. • First epidemiological analyses indicate incidence estimates similar to the US, but comparatively high for Europe. • Clinical trials select considerably younger and preferably male patients with a more benign prognosis. • First results of the treatment survey indicate room for improvement.
The European CML Registry Group in Munich D. Lindörfer M. Pfirrmann, Dipl.Stat., M.Sc., Dr. rer.biol.hum. J. Hasford, Prof. Dr.
Joerg Hasford, MD • Ludwig-Maximilians University • Munich, Germany