Download
1 / 1
10 likes | 77 Views
Explore the barriers and facilitators to early breastfeeding initiation in Ghana through qualitative case histories of postpartum women. Study highlights reasons for delayed initiation and the impact on neonatal mortality rates.

E N D
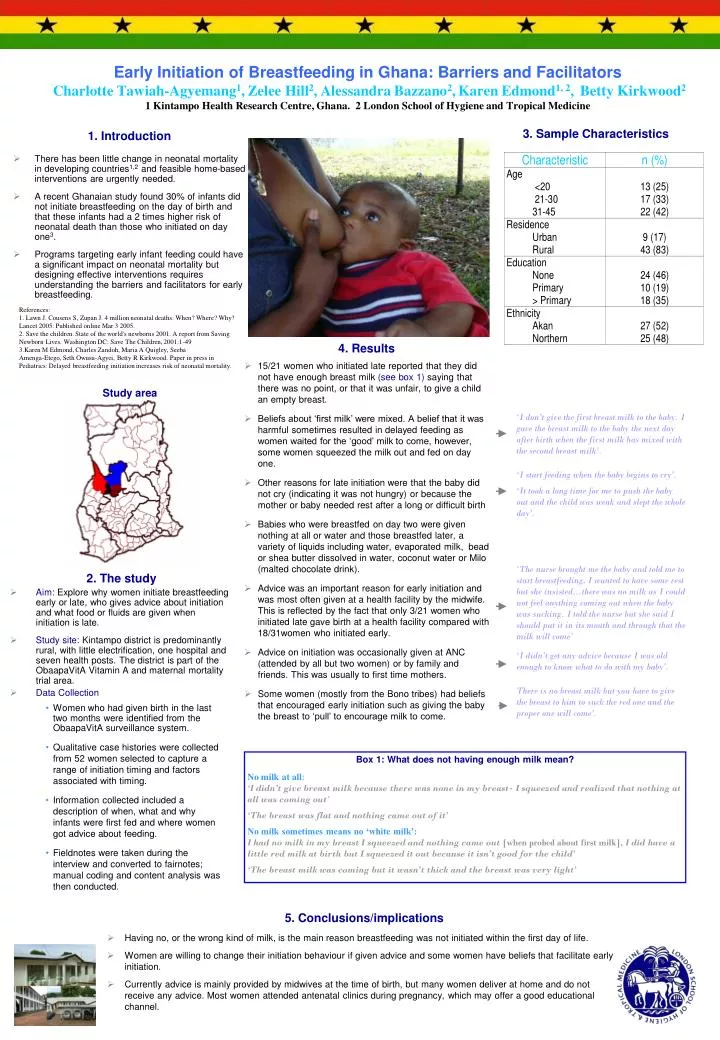
Early Initiation of Breastfeeding in Ghana: Barriers and FacilitatorsCharlotte Tawiah-Agyemang1, Zelee Hill2, Alessandra Bazzano2,Karen Edmond1, 2, Betty Kirkwood21 Kintampo Health Research Centre, Ghana. 2 London School of Hygiene and Tropical Medicine • Women who had given birth in the last two months were identified from the ObaapaVitA surveillance system. • Qualitative case histories were collected from 52 women selected to capture a range of initiation timing and factors associated with timing. • Information collected included a description of when, what and why infants were first fed and where women got advice about feeding. • Fieldnotes were taken during the interview and converted to fairnotes; manual coding and content analysis was then conducted. 2. The study • Aim: Explore why women initiate breastfeeding early or late, who gives advice about initiation and what food or fluids are given when initiation is late. • Study site:Kintampo district is predominantly rural, with little electrification, one hospital and seven health posts. The district is part of the ObaapaVitA Vitamin A and maternal mortality trial area. • Data Collection 1. Introduction • There has been little change in neonatal mortality in developing countries1,2 and feasible home-based interventions are urgently needed. • A recent Ghanaian study found 30% of infants did not initiate breastfeeding on the day of birth and that these infants had a 2 times higher risk of neonatal death than those who initiated on day one3. • Programs targeting early infant feeding could have a significant impact on neonatal mortality but designing effective interventions requires understanding the barriers and facilitators for early breastfeeding. 3. Sample Characteristics References: 1. Lawn J. Cousens S, Zupan J. 4 million neonatal deaths: When? Where? Why? Lancet 2005: Published online Mar 3 2005. 2. Save the children. State of the world's newborns 2001. A report from Saving Newborn Lives. Washington DC: Save The Children, 2001:1-49 3.Karen M Edmond, Charles Zandoh, Maria A Quigley, SeebaAmenga-Etego, Seth Owusu-Agyei, Betty R Kirkwood. Paper in press in Pediatrics: Delayed breastfeeding initiation increases risk of neonatal mortality. • 4. Results • 15/21 women who initiated late reported that they did not have enough breast milk (see box 1) saying that there was no point, or that it was unfair, to give a child an empty breast. • Beliefs about ‘first milk’ were mixed. A belief that it was harmful sometimes resulted in delayed feeding as women waited for the ‘good’ milk to come, however, some women squeezed the milk out and fed on day one. • Other reasons for late initiation were that the baby did not cry (indicating it was not hungry) or because the mother or baby needed rest after a long or difficult birth • Babies who were breastfed on day two were given nothing at all or water and those breastfed later, a variety of liquids including water, evaporated milk, bead or shea butter dissolved in water, coconut water or Milo (malted chocolate drink). • Advice was an important reason for early initiation and was most often given at a health facility by the midwife. This is reflected by the fact that only 3/21 women who initiated late gave birth at a health facility compared with 18/31women who initiated early. • Advice on initiation was occasionally given at ANC (attended by all but two women) or by family and friends. This was usually to first time mothers. • Some women (mostly from the Bono tribes) had beliefs that encouraged early initiation such as giving the baby the breast to ‘pull’ to encourage milk to come. Study area ‘I don’t give the first breast milk to the baby. I gave the breast milk to the baby the next day after birth when the first milk has mixed with the second breast milk’. ‘I start feeding when the baby begins to cry’. ‘It took a long time for me to push the baby out and the child was weak and slept the whole day’. ‘The nurse brought me the baby and told me to start breastfeeding, I wanted to have some rest but she insisted…there was no milk as I could not feel anything coming out when the baby was sucking. I told the nurse but she said I should put it in its mouth and through that the milk will come’ ‘I didn’t get any advice because I was old enough to know what to do with my baby’. There is no breast milk but you have to give the breast to him to suck the red one and the proper one will come’. Box 1: What does not having enough milk mean? No milk at all: ‘I didn’t give breast milk because there was none in my breast- I squeezed and realized that nothing at all was coming out’ ‘The breast was flat and nothing came out of it’ No milk sometimes means no ‘white milk’: I had no milk in my breast I squeezed and nothing came out [when probed about first milk], I did have a little red milk at birth but I squeezed it out because it isn’t good for the child’ ‘The breast milk was coming but it wasn’t thick and the breast was very light’ • 5. Conclusions/implications • Having no, or the wrong kind of milk, is the main reason breastfeeding was not initiated within the first day of life. • Women are willing to change their initiation behaviour if given advice and some women have beliefs that facilitate early initiation. • Currently advice is mainly provided by midwives at the time of birth, but many women deliver at home and do not receive any advice. Most women attended antenatal clinics during pregnancy, which may offer a good educational channel.