Download
1 / 1
10 likes | 75 Views
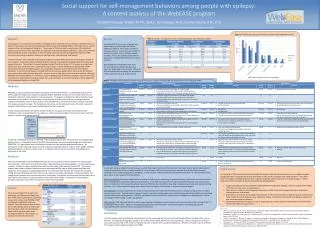
This study examines the impact of socio-demographic factors on epilepsy self-management, healthcare use, and outcomes. Initial findings show correlations between self-management levels and factors like social support and income. The study includes data from a public hospital clinic serving low-income, uninsured patients. Data collection methods, analysis plans, and limitations are discussed.

E N D
Socio-Demographic Differences in Self-Management and its Impact on Healthcare Use and Outcomes in Epilepsy C Begley, PhD1; R Shegog, PhD1; K Talluri, MBBS1; C Chen, PhD1; M Newmark, MD2; S Dubinsky, RN, MPH2; F Barnwell MD3; R Wright, RN3; R Basu, PhD1;D Lairson, PhD1; T Reynolds MS1 1THE UNIVERSITY OF TEXAS SCHOOL OF PUBLIC HEALTH, 2KELSEY-SEYBOLD CLINIC, 3BAYLOR COLLEGE OF MEDICINE Results cont’d Table 5: Correlation between antecedent factors, quality of life (QOLIE) & self-management • Discussion cont’d • Females reported higher levels of self-management than males. • Participants reporting income below $30,000 had higher levels of self management. • Tests of association between self-management, antecedent factors, healthcare use , and quality of life are very preliminary and possibly distorted by the small sample size. • Self-management was positively correlated with social support (p=.03) and outcome expectations (p=.06). • Higher levels of self-management were also correlated with ER visits (p=.07) and hospital admissions (p=.000). • Conclusions • The main limitation of the results so far is the small of number of patients that have completed the self-management questionnaire. • A limitation of the study design is that the self-management information is being obtained during the months following the year in which health care use, and outcome data were collected. • The next steps are to complete the data collection process and merge the self-management database with the existing data on the patients. • Data analysis will proceed from simple univariate descriptive statistics, through multivariate regression and formal hypothesis testing. • We will apply structural equation modeling as our analysis plan in testing hypotheses. • Methods cont’d • The Ben Taub General Hospital (BT) is one of two public general hospitals in Houston that serve about 275,000 primarily low-income, uninsured • and Medicaid-covered patients a year. The hospital-based epilepsy clinic primarily serves Hispanics and black adults. Many patients are also managed by a primary physician in one of 11 community health centers operated by the public hospital system. • Quarterly interviews were conducted over one year from January 2006 through August 2008 on socio-demographic characteristics, clinical condition, healthcare use, and quality of life. • Methods and measures are described in • C Begley et al. Sociodemographic disparities in epilepsy care: Results from the Houston/New York City health care use and outcomes study. Epilepsia.Published Online: Nov 19 2008. • Self-management antecedents, measures, and scales were selected on the basis of an extensive review of the literature and consultation with experts • A self-administered questionnaire was developed addressing self-management, and eight possible antecedents including: knowledge, self-efficacy, control, stigma, social support, depression, patient satisfaction, and outcome expectations (Table 1). • Follow-up interviews on self-management began in October 2008 and are continuing. • Discussion • A total of 29 patients have completed the self-management questionnaire so far. • The participants had a mean age of 42.3 (SD= 14.9). • Almost 70% were female. • They were diverse with regard to race-ethnicity. • The majority (55.1%) were not married. • Most (58.6%) had attended college. • Of those who attended college, about half (47.6%)had obtained a college degree. • The majority of participants (55.1%) were employed full- or part-time. • About one-third (31.0%) reported income of $30,000 or less. • About one-quarter (24.1%) reported income of $70,000 or more. • Almost two-thirds had private insurance (65.5%), 20.7% had public coverage, and 13.8% were uninsured. • The average age when participants were first diagnosed with seizures was 21.3 years and participants had had seizures for an average of 19.6 years (SD=16.1). • Most participants ( 62.1%) reported having had a seizure within the past year. • More than two-thirds (72.4%) of participants reported some form of generalized seizure either as a primary or as a secondary type. • Tests of association between self-management, socio-demographic and seizure characteristics are very preliminary and may be distorted due to the small sample size. • Except for gender and income, there were no statistically significant differences comparing mean self-management scores with socio-demographic and seizure-related characteristics. Results Table 2: Personal characteristics Table 3: Seizure-related variables • Introduction • Self-management is an imperative for patients with epilepsy. • A range of possible antecedent factors have been associated with epilepsy self-management (Fig. 1) • predisposing factors – provide a rationale or motivation for the behavior • enabling factors – enable a motivation to be realized • reinforcing factors – provide continuing reward or incentive for the behavior. • The association between antecedent factors and self-management is beginning to be understood. • The relationship between self-management and healthcare use and outcomes is less known. • The socio-demographic variation in self-management is poorly understood. • Objectives • To determine the relative importance of antecedent factors in predicting self-management. • To determine the relationship between self-management, healthcare use, and quality of life. • To determine differences across socio-demographic groups in self-management, the antecedent factors associated with self-management, healthcare use and quality of life. • This report describes the process developed to measure self-management and its antecedents and presents preliminary data from a sample of 29 patients. • Methods • The project is following a cohort of 430 epilepsy patients at two epilepsy clinics in Houston, Texas • Kelsey-Seybold Clinic isa large multi-specialty medical organization in Houston with 22 clinics and over 300 physicians. Patients are largely from middle-class, employed, populations with private insurance coverage primarily through HMO- or PPO-type plans. Epilepsy patients are referred to a specialty clinic location where there are three general neurologists, one epileptologist, and a nurse epilepsy specialist. Table 4: Comparison of mean self-mgmt. scores by selected variables Table 6: Correlation between self-management and healthcare use variables Figure 1: Framework for Epilepsy Self-Management & Outcomes Table 1: Variables and Scales of Epilepsy Self-Management • Self-Management Behaviors • Treatment management • Keep health care appointments • Take AED medication as prescribed • Seizure management • Call health care professional in an acute situation • Communicate with family members and health care providers • First aid activities – recognizing status epilepticus • Lifestyle management • Changing lifestyle to avoid seizures • Planned disclosure to others • Develop a social support network • Develop linkage to resources • Antecedent Factors • Predisposing factors • Knowledge • Self-efficacy • Control • Stigma • Social support • Depression • Outcome • expectations • Enabling factors • Socio-demographics • Reinforcing factors • Patient satisfaction • Clinical and Health Outcomes • AED blood levels • Seizure frequency • Perceived impact of epilepsy on everyday life • Quality of Life • Functional status • Healthcare Use • AED use • Physician visits • ER visits • Hospitalization Acknowledgments This project is supported by a U.S. Centers for Disease Control and Prevention grant, CDC SIP-06. The authors are particularly grateful to Rosemarie Kobau at the CDC for facilitating the project and to Colleen DiIorio for providing technical assistance. We would also like to thank Stephanie Dubinsky and Raquel Wright for their assistance in conducting patient interviews.